1 in 9
U.S. children ever diagnosed with ADHD
CDC, 2024 (NSCH 2022)
15.5M
U.S. adults currently diagnosed with ADHD
CDC NCHS Rapid Surveys, 2024
3:1
Boy-to-girl diagnosis ratio in childhood – narrowing to 1:1 in adulthood
The Lancet Psychiatry
50–75%
of girls with ADHD are missed in childhood
Capital Area Pediatrics / Mowlem et al.
What Is ADHD?
Attention-Deficit/Hyperactivity Disorder is a neurodevelopmental condition that affects how the brain regulates attention, impulse control, and activity. It is not a problem of intelligence, willpower, or upbringing.
At its core, ADHD involves differences in the brain’s executive function networks – the systems that govern focus, working memory, planning, and self-regulation. These differences are present from early childhood and persist across the lifespan, though how they show up changes with age and environment.
ADHD is highly heritable. If a first-degree relative has ADHD, a child’s risk rises substantially. It occurs across every country, culture, and intelligence level studied. Boys are diagnosed more often in childhood, but adult prevalence rates are roughly equal – meaning girls and women are being missed, not spared.
“ADHD is a persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development. Several symptoms must be present prior to age 12, occur in two or more settings, and clearly interfere with social, academic, or occupational functioning.”
– DSM-5-TR (American Psychiatric Association, 2022)
Executive Function Difference
The frontal-striatal and frontal-parietal networks regulate attention, working memory, and inhibition. In ADHD, these systems develop differently.
Lifelong, Not Outgrown
Roughly two-thirds of children with ADHD continue to meet criteria in adulthood. Hyperactivity may quiet down; inattention and emotional dysregulation often persist.
Strongly Heritable
Twin studies place heritability of ADHD at approximately 74%, among the highest of any psychiatric condition. Genetics matters, but expression depends on environment.
Treatable, Not Curable
With combined behavioural, educational, and (where appropriate) medical support, most people with ADHD see significant gains in function, mood, and outcomes.
How Common Is ADHD?
ADHD is one of the most common neurodevelopmental conditions worldwide. The latest meta-analyses confirm it is not “rising” – it is being recognised in populations who were missed for decades.
11.4%
of U.S. children aged 3–17 have ever been diagnosed with ADHD – about 7 million children
Danielson et al., 2024 (CDC NSCH)
6.0%
of U.S. adults currently diagnosed – 15.5 million people, climbing post-2020
Staley et al., MMWR 2024
4.6%
global pooled adult prevalence post-2020, up from 3% in earlier estimates
King’s College London review, 2025
7.2%
global pooled prevalence in children – roughly 129 million children worldwide
Thomas et al., meta-analysis (175 studies)
The Three Faces of ADHD
DSM-5-TR recognises three presentations. The same person can shift between the across years – childhood hyperactivity often gives way to adult inattention.
Predominantly Inattentive
Difficulty sustaining attention, following through on tasks, organising work, and holding information in mind. Often quiet, internally distracted, daydreamy. Most commonly missed in girls and women.
Danielson et al., 2024 (CDC NSCH)
Predominantly Inattentive
Difficulty sustaining attention, following through on tasks, organising work, and holding information in mind. Often quiet, internally distracted, daydreamy. Most commonly missed in girls and women.
Danielson et al., 2024 (CDC NSCH)
Predominantly Hyperactive – Impulsive
Restlessness, fidgeting, blurting out, interrupting, difficulty waiting. More common in young children and more visible to teachers and parents – leading to earlier referral.
~10% of ADHD diagnoses
How ADHD Shows Up Across the
Lifespan
Symptoms shift with age, gender, and environment. Early identification at any stage opens the door to effective support.
Early Signs (Ages 3–5)
ADHD rarely appears overnight. In preschoolers, the signs are typically intense activity levels, regulation struggles, and difficulty with the basics of structured play. These are risk signals – not diagnoses — and warrant a watchful eye, particularly with family history
Constant motion, climbing or running in inappropriate situations
Difficulty waiting turn, frequent interrupting in play or conversation
Short attention span even for activities the child enjoys
Big emotional reactions out of proportion to triggers
Trouble following simple two-step instructions
Sleep difficulties, often falling asleep late and waking tired
Most Common Early Signals
School-Age Signs (Ages 6–12)
Once formal schooling demands sustained attention, ADHD becomes far more visible. Per CDC guidance, behavioural patterns that show up consistently across two or more settings (home, school, peers) for at least six months are the threshold for clinical concern
Difficulty staying seated, focused, or following multi-step instructions
Frequent careless errors in schoolwork despite knowing the material
Forgetting books, homework, lunchboxes — losing things repeatedly
Avoiding tasks that require sustained mental effort
Talking excessively, blurting answers, interrupting peers
Strong performance on interest-driven tasks; collapse on tasks they find boring
Friction with teachers framed as “not trying” or “doesn’t care”
Reported Challenges in School-Age Children with ADHD
Teen & Adult Signs
ADHD does not vanish with age. Visible hyperactivity quiets. Inattention, emotional dysregulation, and executive function struggles intensify under the demands of independence. Late identification is the norm, not the exception – and still highly valuable
Chronic procrastination on tasks that aren’t urgent or interesting
Time blindness — meetings missed, deadlines underestimated
Internal restlessness even when sitting still
Rejection sensitivity and intense emotional reactions to perceived criticism
Patterns of starting projects with high energy then abandoning them
Burnout from sustained masking; exhaustion at the end of a “normal” day
Higher rates of anxiety, depression, sleep problems, substance use
Adult ADHD Self-Reported Impact
The Three Core Executive Function Deficits
Decades of neuroimaging and cognitive research, summarised by Russell Barkley and the CDC, point to three executive systems that operate differently in ADHD brains.
01
Response Inhibition
The capacity to pause before acting – to stop a thought, an impulse, or a behaviour before it escapes. Weak inhibition shows up as blurting, interrupting, impulsive decisions, and difficulty waiting. It is the most upstream of the executive functions.
The pause that fails02
Working Memory
The mental whiteboard that holds instructions, intentions, and partial calculations while you act on them. In ADHD, the whiteboard wipes early. Multi-step directions, mental math, and “I’ll do it in a minute” routinely collapse.
The whiteboard that wipes01
Self-Regulation of
Attention & Affect
The system that directs attention to what matters, sustains it through boredom, and dials emotional intensity up or down. In ADHD it operates on interest rather than importance – and emotional reactions arrive faster and louder than peers.
Interest, not importanceADHD Rarely Travels Alone
Children with ADHD almost always carry at least one additional condition. Screening for ADHD without screening for what travels with it misses most of the picture – and most of the levers for support.
Anxiety, learning differences, and emotional dysregulation are the most common companions. They amplify each other: a child who can’t focus often can’t read fluently, which feeds frustration, which feeds avoidance, which looks like more ADHD.
~45%
of children with ADHD also have a learning disability (compared with ~5% of children without ADHD)
3×
higher risk of an anxiety disorder in children with ADHD compared with neurotypical peers
42%
of children with autism also meet criteria for ADHD – combined screening matters
What Actually Works
The American Academy of Pediatrics and NICE guidelines converge: combined behavioural, educational, and (where appropriate) medical support consistently outperforms any single approach. Early support changes the trajectory.
01
Externalise the Executive Function
Put working memory outside the head. Visual schedules, checklists, timers, and structured routines do the cognitive work the brain struggles to do internally.
02
Behavioural Parent Training
First-line intervention for children under six per AAP guidelines. Teaches consistent consequences, scaffolded routines, and the regulation skills children with ADHD don’t pick up on their own.
03
Classroom Accommodations
Preferential seating, movement breaks, chunked instructions, extended time, and quiet test settings. These aren’t advantages – they level the playing field for executive load.
04
Cognitive Behavioural Therapy
For adolescents and adults, CBT adapted for ADHD targets time blindness, procrastination, emotional reactivity, and the negative self-talk built up from years of unrecognised struggle.
05
Medication, When Indicated
Stimulants remain the most effective treatment for moderate-to-severe ADHD, with roughly 70–80% response rates. Non-stimulants offer alternatives. Always clinician-led, never first without behavioural foundations.
06
Sleep, Movement, Nutrition
Not cures, but powerful amplifiers. Consistent sleep, daily aerobic movement, and stable blood sugar materially reduce ADHD severity scores and improve everything else that follows.
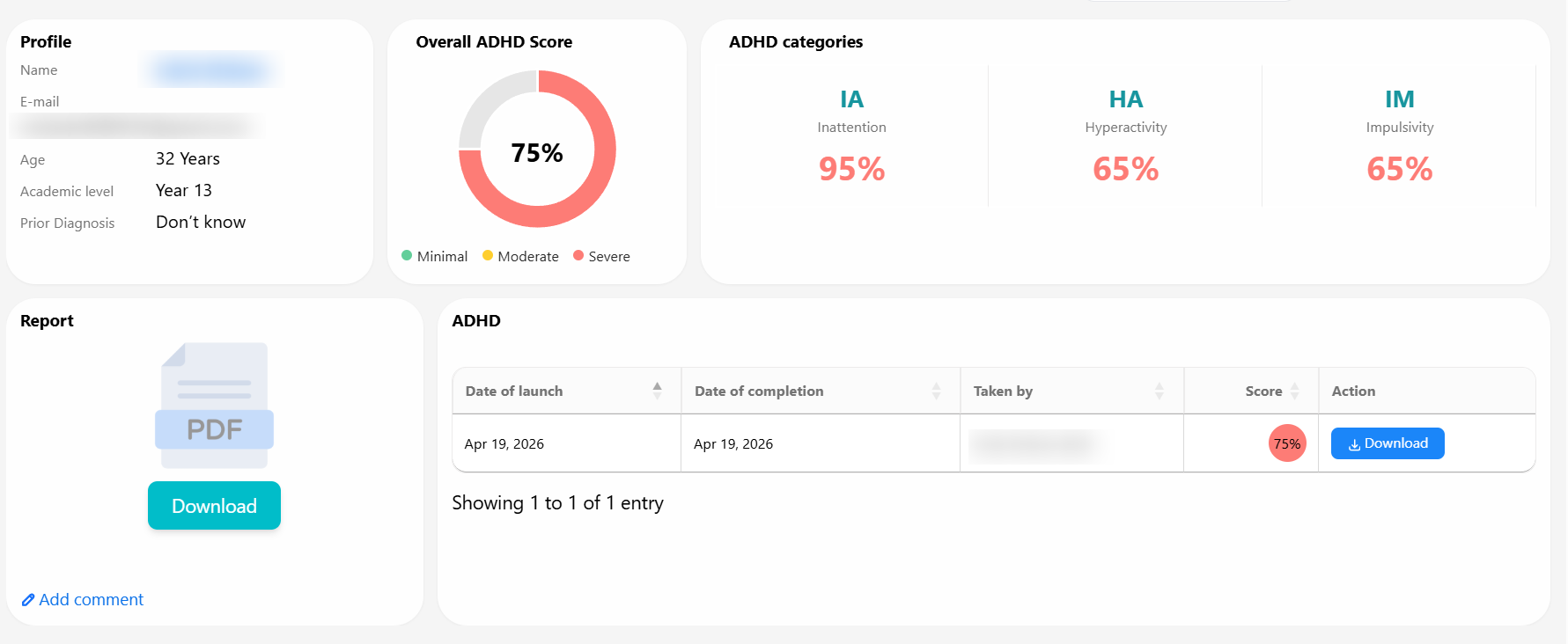
ADHD Screening & Assessment
From a quick free check to a clinician-grade assessment – choose what fits your situation.
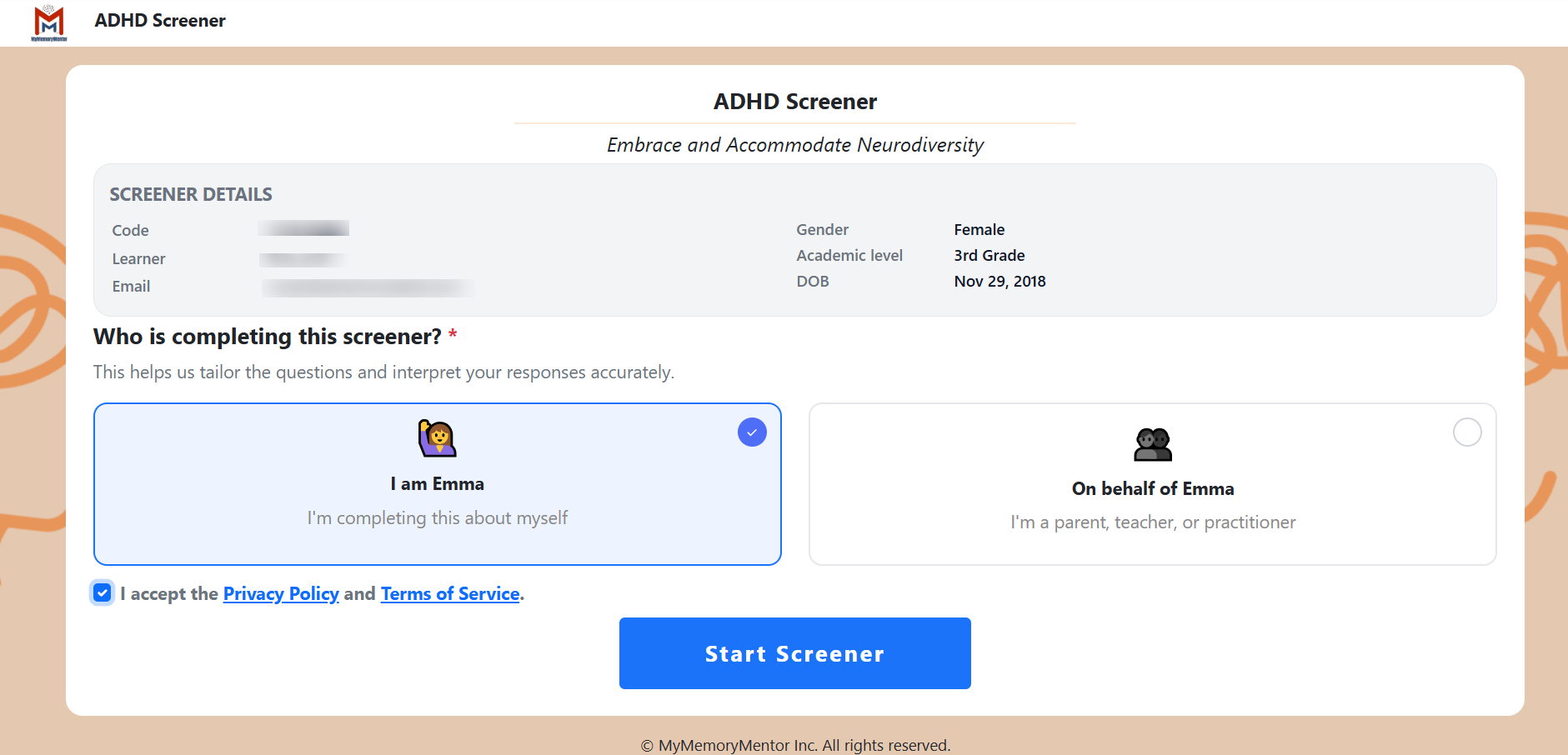
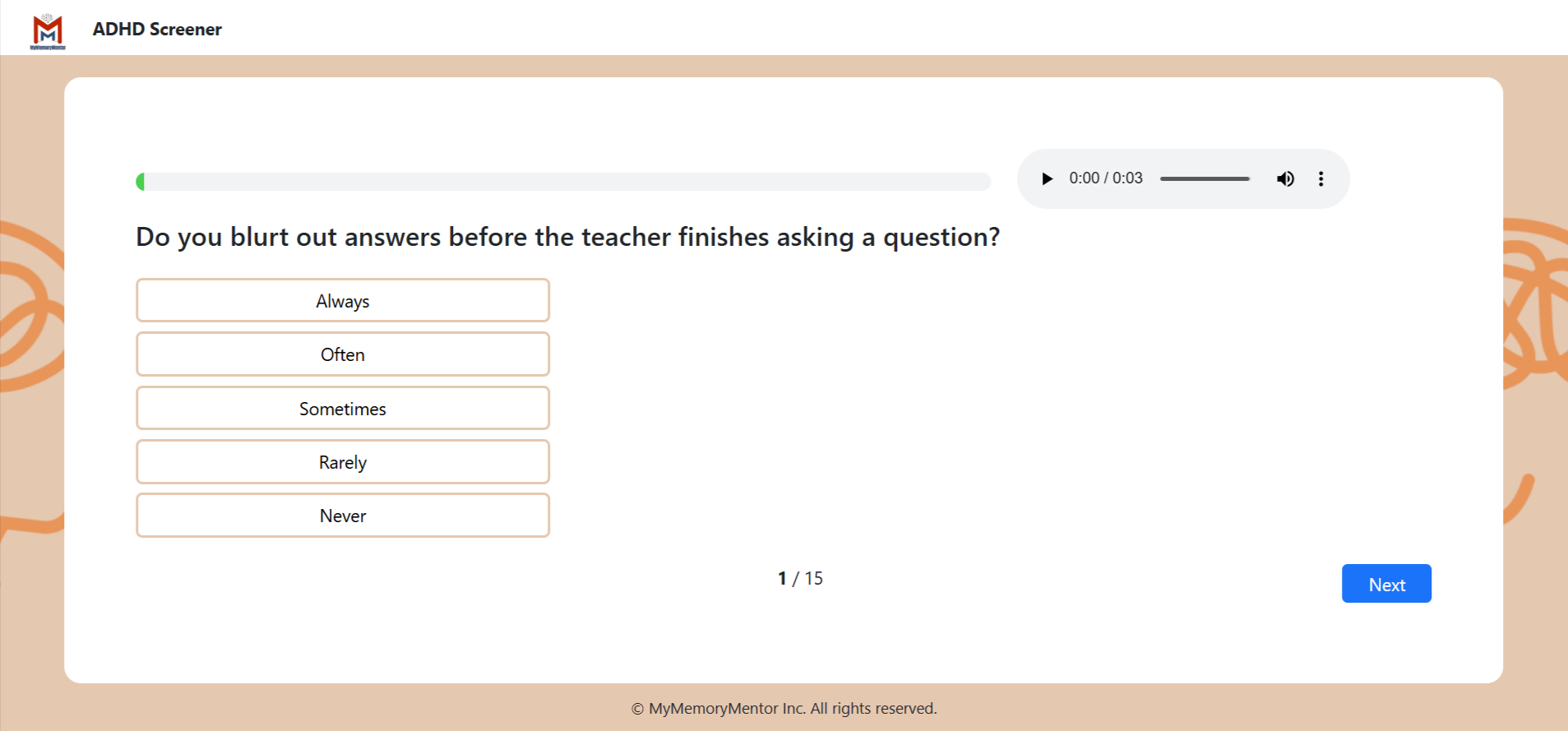
Free ADHD Symptom Screener
A fast, validated questionnaire mapped to DSM-5-TR criteria for inattention and hyperactivity-impulsivity. Ideal for parents, teachers, adults, and self-referral.
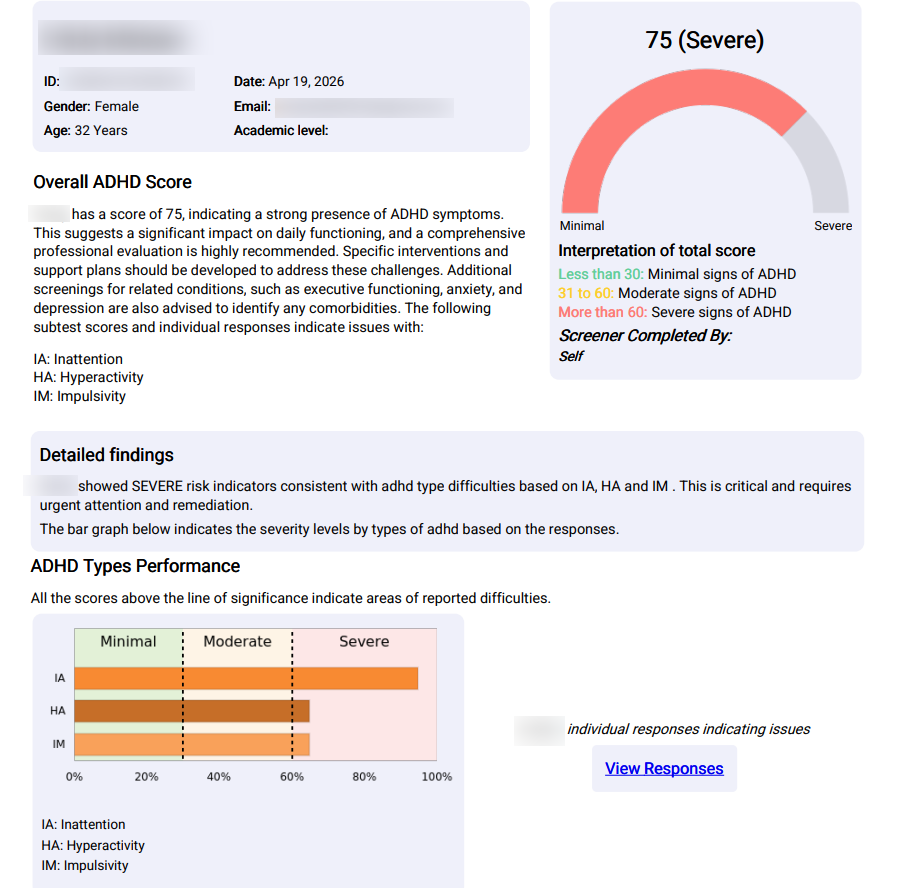
Full ADHD Assessment
A psychometrically validated multi-rater assessment measuring inattention, hyperactivity-impulsivity, executive function, emotional regulation, and functional impairment – producing a full diagnostic-grade profile.
ADHD Myths vs. Facts
Misconceptions delay identification. Here’s what the research actually shows.
Myth
“ADHD isn’t a real condition — it’s just modern parenting.”
Fact
ADHD is one of the most well-validated conditions in psychiatry, with consistent neuroimaging, genetic, and longitudinal evidence across 60+ years of research. Heritability sits around 74%.
Myth
“Children outgrow ADHD.”
Fact
Roughly two-thirds of children with ADHD continue to meet criteria as adults. Hyperactivity may quiet; inattention and emotional dysregulation persist. Adult ADHD is not adult-onset – it is unrecognised childhood ADHD.
Myth
“ADHD only affects boys.”
Fact
Adult diagnosis rates are nearly equal between men and women. The childhood 3-to-1 boy-girl ratio reflects under-referral of girls, not lower prevalence. As many as 50 to 75 percent of girls with ADHD are missed.
Myth
“If they can focus on games or YouTube, they don’t have ADHD.”
Fact
ADHD is an attention regulation difference, not an attention absence. The brain runs on interest, novelty, and urgency. The same person who can hyperfocus for hours on a passion can struggle to start a five-minute task they find boring.
Myth
“ADHD medication leads to substance abuse.”
Fact
The opposite holds in the research. Properly treated ADHD lowers substance use risk by approximately 30 to 60 percent compared to untreated ADHD. The risk lies in non-treatment, not in treatment.
Myth
“It’s too late to get assessed as an adult.”
Fact
Adult diagnosis transforms outcomes – relationally, professionally, and emotionally. Many adults describe diagnosis as the first time their life made coherent sense. The right strategies and accommodations work at any age.
Start Identifying ADHD Today
A free screening takes less than 10 minutes and can provide real clarity. Early identification changes outcomes – for children, teenagers, and the adults who quietly suspected for years.