1 in 31
U.S. children identified with autism – highest rate ever recorded
CDC ADDM Network, MMWR April 2025
1 in 20
prevalence among U.S. boys; 1 in 70 among girls (likely under-reported)
CDC ADDM 2025
1 in 12.5
prevalence in California – highest of any U.S. state
HHS / CDC, April 2025
~5×
increase in identified prevalence since CDC surveillance began in 2000
CDC ADDM longitudinal data
Autism reshapes every academic outcome – even when the child looks like they are coping.
3.5×
more boys diagnosed than girls
The 3.5-to-1 ratio reflects under-referral of girls, not lower prevalence. Girls mask through mimicry, friendship-group attachment, and academic compliance – so the autism hides for years behind exhaustion and anxiety.
~36%
have IQs above 85
Roughly a third of identified autistic children have average-to-superior intelligence. They are the ones most often dismissed with “they can’t be autistic – look at their grades.” Yet their academic effort costs three times what peers spend.
~80%
experience masking-related burnout
Years of camouflaging autism in school produces meltdowns at home, school refusal in secondary years, and adult mental health diagnoses (anxiety, depression, eating disorders) layered on top of unrecognised autism.
What Is Autism?
Autism Spectrum Disorder is a lifelong neurodevelopmental condition that shapes how a person communicates, experiences sensory input, processes social information, and navigates change. It is not a disease, not a tragedy, and not something a person grows out of. It is a different operating system, with its own strengths and its own real costs in environments designed for neurotypical brains.
Autistic individuals can be brilliant pattern-thinkers, deeply ethical, exceptionally focused, and creatively original. They can also be exhausted by sensory environments most people barely notice, fatigued by the constant social translation that school and work demand, and misunderstood by adults who confuse compliance with comfort.
Autism runs in families. It is one of the most heritable conditions in psychiatry. Early identification matters – not because autism needs to be cured, but because the right supports, accommodations, and self-understanding change the trajectory entirely.
“Autism is characterised by persistent deficits in social communication and social interaction across multiple contexts, along with restricted, repetitive patterns of behaviour, interests, or activities. Symptoms must be present in the early developmental period and cause clinically significant impairment in social, occupational, or other important areas of current functioning.“
– DSM-5-TR, American Psychiatric Association (2022)
A Spectrum, Not a Scale
Autism is multi-dimensional. Two autistic people may share almost nothing in surface presentation. The DSM-5-TR severity levels reflect support needs, not “how autistic” someone is.
Highly Heritable
Twin studies place autism heritability at 64-91%. If one identical twin is autistic, the other has roughly a 70% chance of being autistic too. Genetics is not destiny, but it is the strongest signal we have.
Sensory at the Core
The DSM-5 explicitly added sensory differences as a diagnostic criterion in 2013. Hyperacusis, light sensitivity, tactile defensiveness, and interoceptive differences are not peripheral – they are the daily reality that drives much of what is observed.
Lifelong, Identifiable Early
Reliable identification is possible from 18 months. Early supports are most effective during the developmental window before age 5, but identification at any age – including adulthood – opens access to understanding and accommodation.
What Autism Gets Called Instead
Autism rarely arrives wearing its own name – especially in girls, high-IQ children, and adults. Because autistic distress shows up through anxiety, exhaustion, school refusal, andquiet underperformance, the diagnostic conversation usually starts somewhere else. Recognising the pattern is the first step toward the right support.
“Anxiety”
Constant low-level worry, tearfulness before school, stomach aches on Sunday nights. Often the first label applied – and often where the conversation stops.
Really → anxiety produced by trying to navigate a sensory and social environment built for neurotypical brains.
“Shy”
Quiet in class, avoids group work, prefers one close friend, melts down at large social events. Often described as mature or well-behaved.
Really → social bandwidth fully consumed by translating unwritten rules others read instinctively.
“Gifted but Lazy”
Brilliant test scorer, abysmal homework completer. The pattern that frustrates teachers and parents because the potential is so visible.
Really → executive function difficulty masked by raw cognitive horsepower until task complexity rises.
“School Refusal”
By Year 7 or 8, the child stops being able to enter the building. Tearful, physically unwell, panic-stricken. Often diagnosed as anxiety disorder.
Really → autistic burnout from years of masking; the nervous system has run out of capacity to cope.
“ADHD” (Only)
50–70% of autistic individuals also have ADHD. Many get only the ADHD diagnosis; the autism is missed because attention symptoms are more visible.
Really → AuDHD — both conditions, requiring both lenses to plan support correctly.
“Depression”
Adolescent withdrawal, flat affect, low energy, suicidality. The mental health diagnosis arrives; the underlying autism never gets explored.
Really → the depression is real and the autism is causing it through years of unrecognised struggle.
“Eating Disorder”
Restrictive eating in autistic girls is increasingly recognised as Avoidant Restrictive Food Intake Disorder (ARFID), often misdiagnosed as anorexia.
Really → sensory sensitivity to texture, smell, temperature – not body image distortion. Different treatment entirely.
“Difficult”
The child everyone describes as challenging, rigid, oppositional, or “always wanting their own way.” The hardest label to peel back.
Really → cognitive inflexibility plus sensory overwhelm – neurology, not personality. The behaviour is the signal.
How Common Is Autism?
Autism rates have risen dramatically over two decades. The CDC’s 2025 ADDM report places U.S. prevalence at 1 in 31 – a 16% rise in two years. Researchers debate whether this reflects true rise or improved identification. What is settled is that autism affectsfar more people than the public, schools, or clinical training systems are currently equipped for.
3.2%
of U.S. 8-year-olds identified with autism – 1 in 31 children
CDC ADDM Network, MMWR April 2025
1 in 26
prevalence among Asian/Pacific Islander children – highest racial/ethnic group
CDC ADDM 2025
~1%
global pooled prevalence – but international identification systems remain underdeveloped
WHO; Lancet Psychiatry global review
~2%
estimated U.S. adult prevalence – most remain undiagnosed
CDC adult ASD research summaries
The Three Levels of Support Need
DSM-5-TR organises autism by support requirements, not by severity of autism itself. The same child may sit at different levels across social communication and restricted, repetitive behaviours. Levels describe where the person needs scaffolding – they do not rank human worth.
Requires Support
Social communication differences are present but masked or compensated. The child may pass as “quirky” or “sensitive” for years. Academic outcomes can be strong with high cognitive cost.
- Danielson et al., 2024 (CDC NSCH)
- Rigidity that interferes with flexibility across contexts
- Often the level missed in girls and high-IQ children
- Significant masking-related fatigue and burnout risk
Requires Substantial Support
Social communication differences are clearly apparent. Restricted interests and repetitive behaviours are visible. Inflexibility produces obvious distress when routines change.
- Marked verbal and nonverbal social communication challenges
- Difficulty changing focus or activity
- Restricted behaviours noticeable to others
- Anxiety and meltdowns more frequent
Requires Very Substantial Support
Severe deficits in verbal and nonverbal communication. Extreme distress at change. High support needs across daily living. Around two thirds of children in the 2025 ADDM cohort had borderline or significant intellectual disability.
- Limited or no verbal communication
- Daily living skills require significant scaffolding
- Sensory needs require structured environments
- Often co-occurring intellectual disability
How Autism Shows Up Across the Lifespan
Autism is identifiable from 18 months. Yet many autistic people – particularly girlsand high-IQ individuals – are not formally identified until adolescence or adulthood. Signs evolve with age, environment, and the cost of masking.
Early Signs (Ages 1–5)
CDC’s “Learn the Signs. Act Early.” programme identifies reliable markers from 18 months. Early identification dramatically improves trajectory – but parents should never wait for certainty. If concern is present, screening is appropriate
Limited or absent eye contact and social smiling
Delayed speech, or speech that develops then regresses
Repeating phrases from videos rather than spontaneous communication
Lining up toys, intense focus on parts of objects
Distress at small environmental changes – clothing, routes, food
Limited pretend play or joint attention with caregivers
Sensory-seeking or sensory-avoiding behaviours (covering ears, tip-toe walking, food refusal)
Most Common Early Identification Signals
School-Age Signs (Ages 6–12)
School makes autistic difference visible – sometimes through obvious markers, often through quieter ones. Girls in particular present a profile that schools historically miss: quiet, academically capable, attached to one or two friends, and falling apart at home while looking fine in the classroom.
Difficulty with group work, unstructured play, or social negotiation
Intense, narrow interests pursued in unusual depth
Rigidity around rules, fairness, routine, schedule changes
Strong vocabulary paired with literal interpretation of language
Meltdowns after school despite “fine” school day
Selective eating, sensory clothing preferences, noise sensitivity
Friendship intensity followed by sudden, baffling fall-outs
Performance gap between effort spent and grades received
Reported Challenges in School-Age Autistic Children
Teen & Adult Signs
Late identification is now the norm rather than the exception, particularly for girls and women. Many adults discover their autism through their own child’s diagnosis. The recognition is rarely a loss – it is the explanation for decades of unexplained exhaustion, social pain, and “trying harder than everyone else just to look normal.”
Persistent social exhaustion – recovering for hours from a “normal” interaction
Lifelong sense of being from a slightly different planet than peers
Career path heavily skewed toward specialist or solo work
Sensory needs around clothing, noise, lighting, food
Conscious, learned scripts for social situations others handle intuitively
Mental health diagnoses (anxiety, depression, OCD) accumulated over years
Burnout episodes that look like depression but follow social or environmental overload
Strong sense of justice, deep ethical thinking, intense focused interests
Adult Autistic Self-Reported ImpacT
The Three Cognitive Domains
Decades of cognitive neuroscience identify three interdependent systems that operate differently in autistic brains. Understanding these explains why an autistic child can excel atone task and collapse at another that looks easier from outside.
01
Social Cognition
The system that infers intention, predicts behaviour, and reads unwritten social rules. In autism, this system processes social information more deliberately and analytically – sometimes accurately, often slowly, and always at higher cognitive cost than for neurotypical peers.
The intuition that costs effort02
Sensory Processing
Recognised in 95% of autistic individuals, sensory differences mean the brain receives, weighs, and filters sensory input differently. Sound, light, touch, temperature, taste – every channel can be amplified, dampened, or processed out of sequence. This is the foundation of much classroom struggle.
The unfilterable signal03
Cognitive Flexibility
The system that shifts attention, switches between tasks, and updates predictions when reality changes. Autistic brains often run more rigid, more pattern-locked, more thorough. The strength: deep focus and pattern recognition. The cost: schedule changes, unexpected questions, and transitions create disproportionate distress.
The depth-over-shift trade-offAutism Rarely Travels Alone
Co-occurring conditions are the rule, not the exception, in autism. Identifying the autism without identifying its companions produces incomplete support. Identifying the companions without recognising the autism produces decades of treating downstream symptoms while the upstream cause goes unaddressed.
The AuDHD profile – autism plus ADHD – is now recognised as a distinct, common presentation. 2025 PMC reviews place co-occurrence between 50 and 70% in either direction. Anxiety, sensory processing disorder, intellectual disability, and learning differences all overlap significantly
~80%
of ADHD cases involve a co-occurring condition -anxiety is the most common
~40%
of autistic children meet criteria for clinically significant anxiety
~50%
of adults with anxiety also experience depression -the most common adult comorbid pair
EMA – Evaluation of Math Ability
A 360° cognitive profile of mathematical learning. For families exploring autism, EMA serves a precise purpose: it reveals whether a child’s academicstruggles stem from cognitive content gaps or from the executive function, sensory processing, and working memory differences that autism produces.
Why EMA matters for autism investigation: Autistic children often present striking cognitive profiles – strong number sense paired with broken proceduralfluency, intact reasoning paired with collapsed working memory under classroom load. EMA’s six domains surface exactly this pattern, separating “they cannot do the maths” from “their executive function cannot hold the maths.”
Number Sense
Foundational understanding of quantities, order, and numerical relationships.
→ Often intact in autistic learners — strong here with weak elsewhere is a signal
Math Facts & Fluency
Automatic retrieval of addition, subtraction, multiplication, and division.
→ Timed fluency often collapses under autism’s working memory load
Visual Processing & Subitising
Visual-spatial and pattern skills critical for quantity perception, geometry, and layout.
→ Autistic strengths in pattern recognition can show here
Working Memory
Capacity to hold and manipulate numbers in mind during multi-step problems.
→ The exact system Pastor-Cerezuela found impaired by sensory load in ASD
Math Reasoning
Application of concepts in word problems and conceptual understanding.
→ Strong logical reasoning paired with collapsed output is highly diagnostic
Rapid Automatised Naming
Speed of visual-verbal association – a shared marker across neurodevelopmental conditions.
→ RAN deficits flag executive function patterns common in autism
The Cognitive Fingerprint Autism Leaves in Mathematics
Research from Pastor-Cerezuela and colleagues confirms that autistic children show predictable executive and cognitive dysfunction in inhibitory control, auditory sustained attention, and short-term verbal memory – driven, in significant part, by atypical sensory processing in classroom environments. The same systems EMA measures.
An autistic child may demonstrate intact number sense and excellent reasoning on the EMA’s untimed conceptual tests, then collapse on rapid automatised naming and timed fluency tasks – not because the maths is missing, but because the cognitive load of timed performance exceeds available bandwidth. That profile is itself a diagnostic signal. It tells parents, teachers, and clinicians: the maths is fine. The system holding the maths is the issue. From there, the support plan can target the right thing.
What Actually Helps
Autism does not need to be cured. It needs to be understood, accommodated, and respected. Evidence-informed support focuses on building self understanding, reducingenvironmental load, teaching practical skills, and amplifying autistic strengths – never on extinguishing autistic identity.
01
Sensory Environment Design
Reduce fluorescent lighting, lower ambient noise, offer noise-cancelling headphones, allow movement breaks, provide quiet spaces. The TEACCH structured teaching model shows that environmental modification alone produces significant gains.
02
Predictability and Visual Structure
Visual schedules, individual work systems, advance warning of transitions. Autistic brains operate well with structure and predictability – these are not crutches, they are the right cognitive scaffolding.
03
Speech and Language Therapy
For children with verbal communication differences, SLT supports both expressive language and pragmatic/social communication. Augmentative and alternative communication (AAC) options where helpful, never as a “last resort.”
04
Occupational Therapy
Sensory integration work, fine motor support, daily living skills, and the practical bridge between autistic perception and everyday environmental demands. Most evidence-based when delivered by OTs with specific autism training.
05
Educational Accommodations
IEP, 504, or EHCP plans covering extended time, alternative testing environments, reduced sensory load, executive function scaffolding, and access to support staff. Backed by IDEA, the UK Equality Act, and equivalent legislation worldwide.
06
Autistic-Led Self-Understanding
The strongest predictor of adult autistic mental health is identity acceptance. Connecting with autistic community, learning about masking and burnout, and unmasking selectively in safe contexts changes long-term outcomes more than any single intervention.
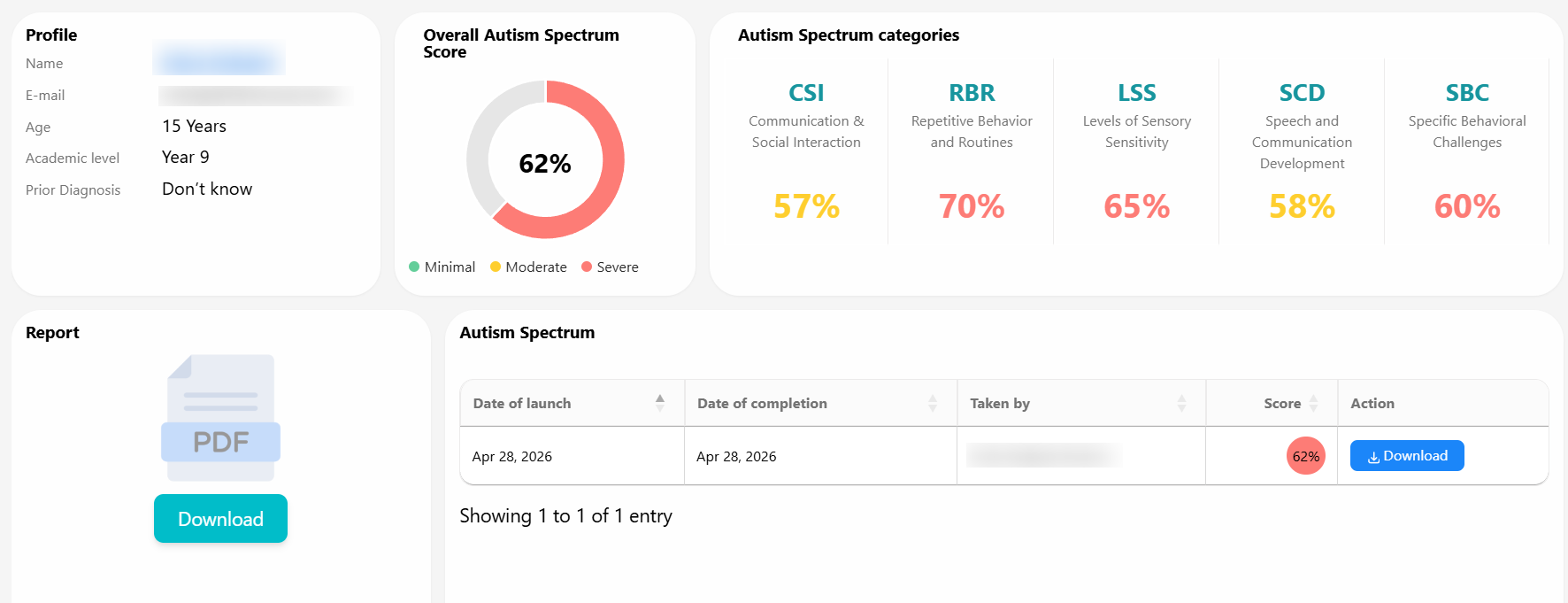
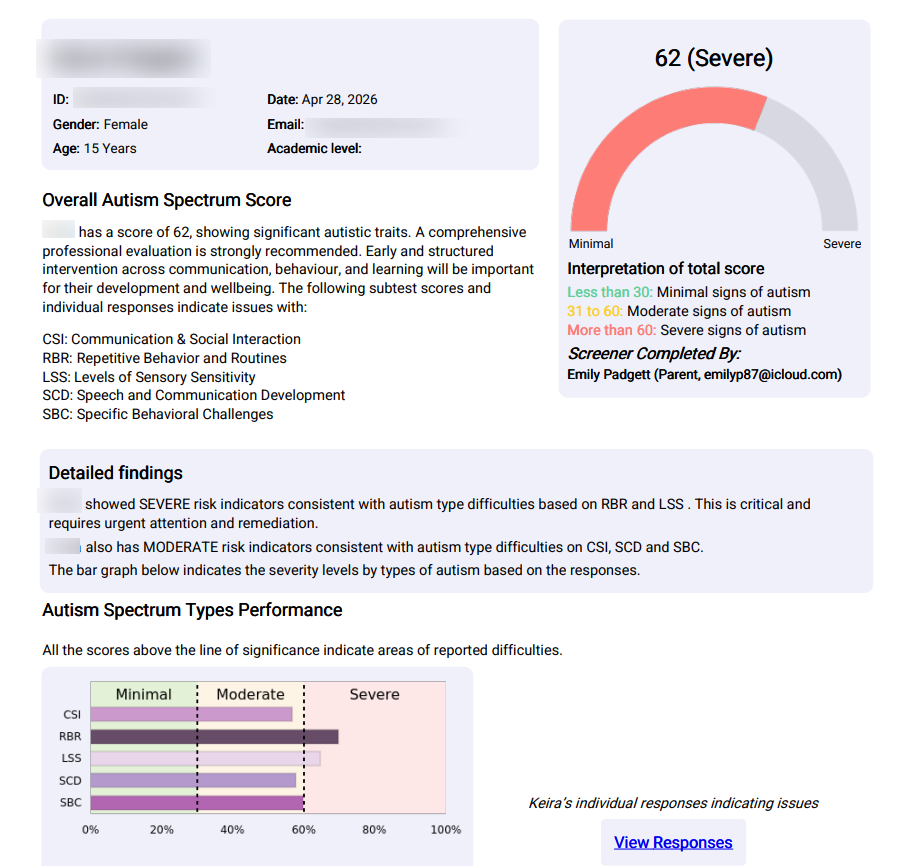
Autism Screening & Assessment
From a quick free screener to EMA, MyMemoryMentor’s comprehensive cognitive assessment that surfaces the executive function and processing patterns autism produces – choose what fits your situation.
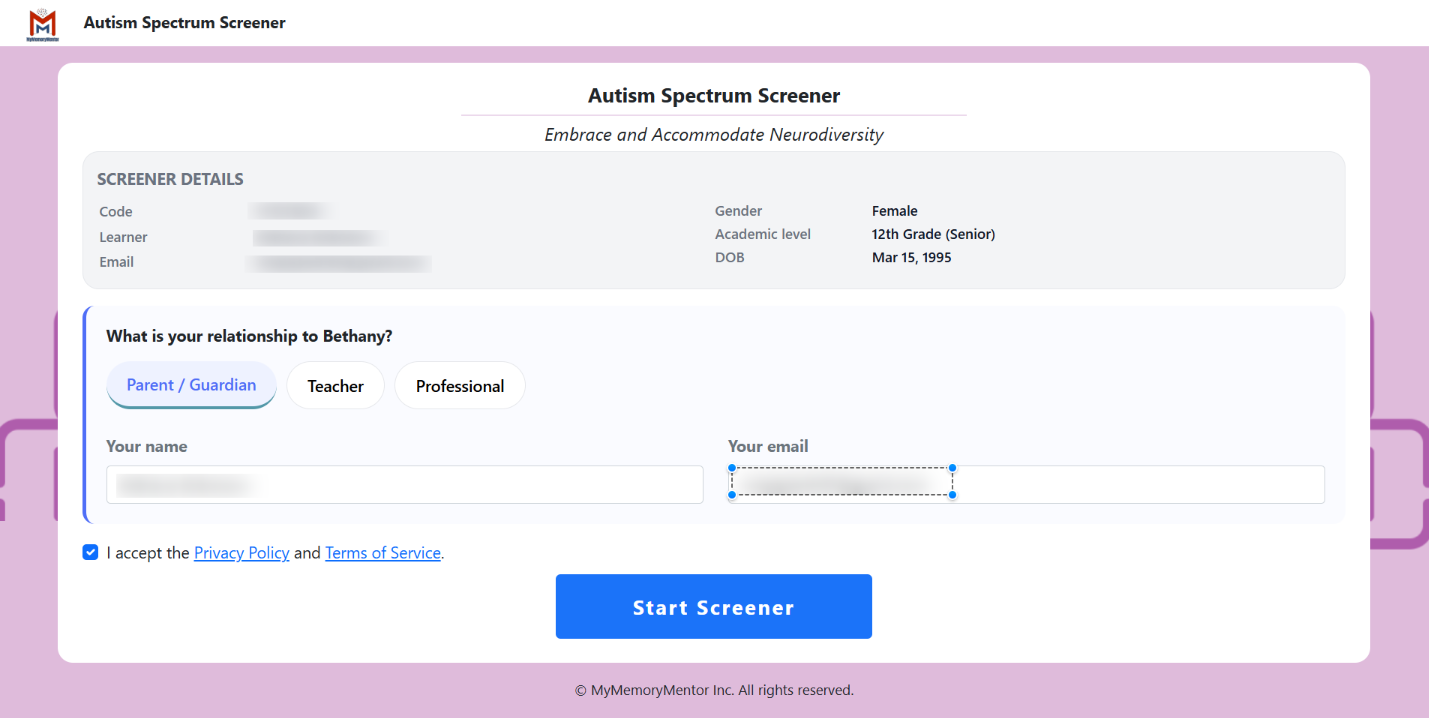
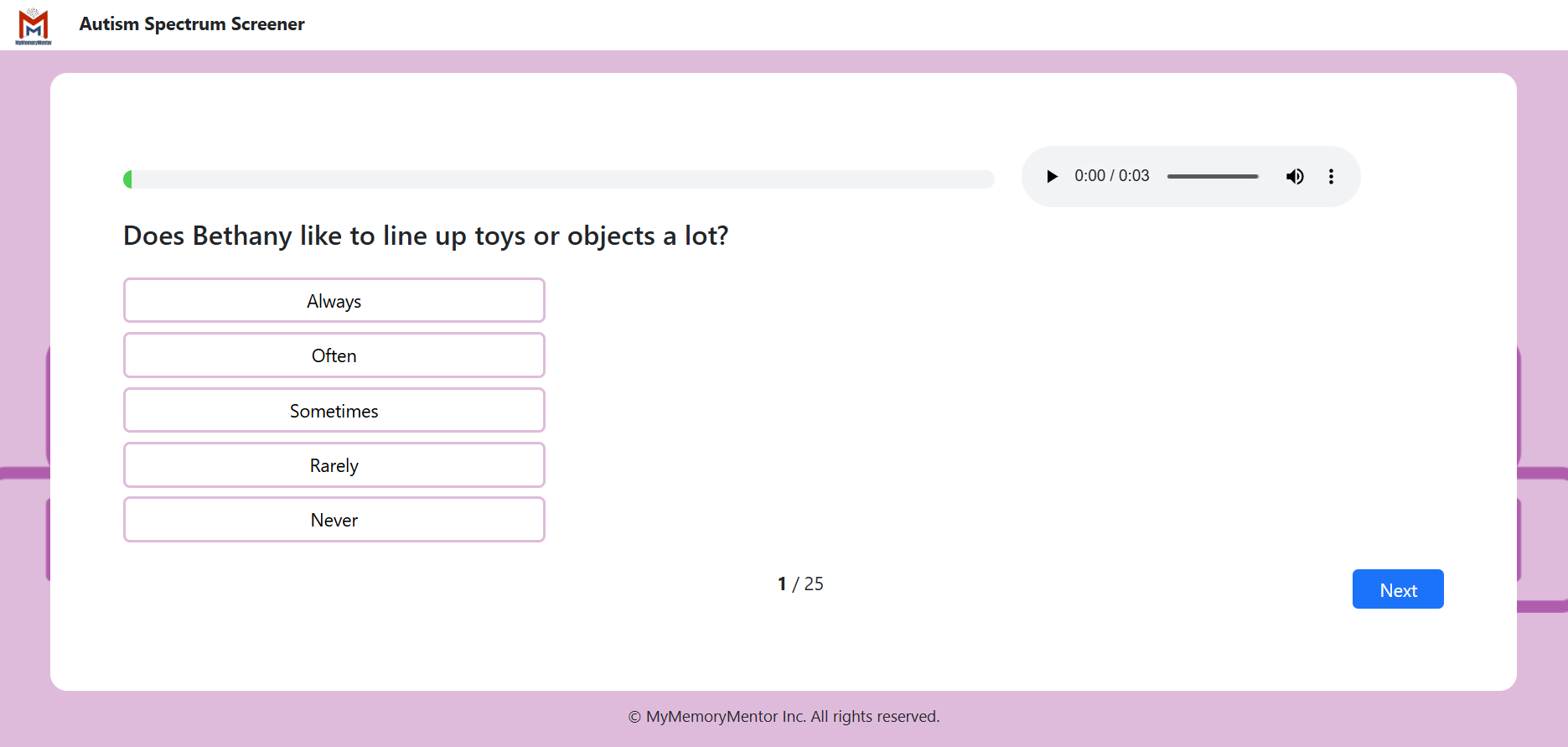
Free Anxiety Screener
A validated questionnaire built on DSM-5-TR criteria with separate male and female presentation profiles. Surfaces social communication patterns, sensory differences, restricted interests, and masking signals across age groups
- Free – no account required to start
- Age-banded versions: early childhood, school age, teen, adult
- Separate sensitivity profiles for masked and overt presentations
- Plain-language results in under 10 minutes
- Flags co-occurring ADHD, anxiety, and learning difference signals
- DSM-5-TR and ICD-11 aligned
MOST COMPREHENSIVE
EMA — Evaluation of Math Ability
MyMemoryMentor’s psychometrically validated comprehensive cognitive assessment. Particularly powerful for autism investigation when academic struggles need cognitive separation – revealing the executive function and processing patterns autism produces in mathematical performance
- Six cognitive domains: number sense, fluency, visual processing, working memory, reasoning, RAN
- Surfaces the cognitive fingerprint of autism in academic output
- Separates content knowledge from executive function and working memory
- Identifies co-occurring learning differences alongside autism
- Suitable for IEP, 504, EHCP, and MTSS/RTI submissions
- Parent- and teacher-friendly report language
- GDPR and HIPAA – aligned data handling
Autism Myths vs. Facts
Misconceptions delay identification by years -sometimes decades. Here is what the research actually shows.
Myth
“They can’t be autistic — they make eye contact and have friends.”
Fact
Many autistic people, especially girls, learn eye contact and friendship patterns through conscious study and mimicry. Masking is exhausting precisely because it works. The presence of “social skills” is not evidence against autism – it is often evidence of high masking effort.
Myth
“Autism is being over-diagnosed.“
Fact
The CDC’s 2025 data shows roughly two-thirds of identified autistic children have borderline or significant intellectual disability – actively contradicting the idea that the rise is just “high-functioning” cases. Girls and ethnic minorities remain systematically under-identified, suggesting current numbers undercount, not overcount.
Myth
“Autism only affects boys.”
Fact
The 3.5:1 boy-to-girl diagnostic ratio reflects assessment tool bias, not biological reality. Standardised tools like ADOS-2 and ADI-R were validated primarily on male samples. Researchers now estimate the true biological ratio is closer to 2:1 or even 1.5:1.
Myth
“They’ll grow out of it.”
Fact
Autism is lifelong. The behavioural presentation may evolve dramatically – particularly with appropriate support – but the underlying neurology persists. Adults do not “stop being autistic.” Many simply become better at masking, often at significant mental health cost.
Myth
“Vaccines cause autism.”
Fact
The original 1998 study has been formally retracted. Subsequent meta-analyses covering millions of children across multiple countries find no causal link. Autism is highly heritable, with brain differences detectable prenatally. The vaccine claim has been comprehensively disproved.
Myth
“A late diagnosis is too late to matter.”
Fact
Research consistently links self-understanding and identity acceptance to dramatically better mental health outcomes in autistic adults. Diagnosis at 14, 30, or 60 opens access to accommodations, community, and the explanation for decades of unspoken struggle. It is never too late.
Stop calling it “just anxiety.”
A free screening takes less than 10 minutes. For families investigating academic struggle that anxiety alone cannot explain, EMA adds the cognitive profile that reveals what the surface scores hide.