#1
leading cause of disability globally by years lived with disability – ahead of all other mental and physical conditions
WHO Global Burden of Disease 2023
25–35%
rise in depression prevalence following the COVID-19 pandemic – particularly in adolescents and young adults
Lancet; Nature Human Behaviour 2022
60%
of people with ADHD also meet criteria for depression – one of the highest overlap rates in psychiatry
Biederman et al.; NIMH 2024
2–3×
higher prevalence in women than men across the lifespan – with adolescent girls at highest risk globally
WHO; APA 2024
Depression is the world’s leading cause of
disability – and it’s most dangerous when no
one names it.
280M
people globally live
with depression
The WHO 2023 World Mental Health Report places depression at 3.8% of the global population – rising to 5.7% among adults over 60. Prevalence is nearly double in women. Post-pandemic estimates from the Lancet and Nature Human Behaviour push the burden 25–35% higher than pre-2020 baselines.
50-80%
of cases remain
undiagnosed or mistreated
Lancet Psychiatry 2023 reviews consistently show that the majority of people with depressive disorder are never accurately identified – particularly in adolescents and older adults. Cognitive symptoms are the most frequently missed, leading to incorrect diagnoses of ADHD, SLDs, or early dementia before the underlying depression is ever named.
7-10 yrs
average delay to first
effective treatment
The global treatment gap for depression is staggering. Across WHO regions, fewer than 25% of people with depressive disorder receive minimally adequate care. In low- and middle-income settings, the gap exceeds 75%. Even in high-income countries, the median time from first symptom to first effective intervention exceeds seven years.
What Is Depression – Really?
Depression is not sadness. Sadness is a temporary emotional response to loss or disappointment. Depression is a persistent neurobiological state that impairs the systems the brain uses for reward, energy, motivation, cognition, and emotional regulation – simultaneously, across every domain of functioning, for weeks or months at a time.
This is the critical distinction that clinicians and families most often miss. Depressive disorder does not always present as crying or visible distress. It frequently presents as flatness, emptiness, chronic exhaustion, the inability to feel pleasure in things that used to matter, slowed thinking, and an erosion of self-worth that the person may have lived with for so long they have accepted it as their personality.
Depression is highly treatable – across therapy modalities, pharmacological support, lifestyle intervention, and structured care planning. The barrier is not treatment. The barrier is accurate identification, which requires moving beyond mood to assess all five domains of depressive functioning.
“Depression is a whole-brain, whole-body condition. Reducing it to ‘feeling sad’ is like reducing a stroke to ‘a bad headache.’ The cognitive, somatic, and self-concept components are not side effects of the mood disturbance. They are core features of the disorder – and they often outlast the mood symptoms themselves.”
– Rush et al., Neurobiological Mechanisms of Unipolar Depression, Nature Reviews Neuroscience 2022
Mood Dysregulation
Persistent low mood, tearfulness, emotional flatness, or irritability lasting two weeks or more – distinct from situational distress.
Anhedonia
Loss of pleasure in previously enjoyed activities – often the most diagnostically specific feature and the first sign in adolescents.
Cognitive Slowing
Concentration impairment, slowed processing speed, memory gaps, and decisional paralysis – frequently confused with ADHD or early cognitive decline.
Somatic Burden
Fatigue, sleep disruption, appetite changes, and psychomotor slowing – physical symptoms that often precede mood symptoms by months.
Five Domains of Depressive Functioning
The MMM Depression Screener maps across five evidence-based domains drawn from DSM-5-TR, ICD-11, and the GRID-HAMD clinical framework. Each domain captures a distinct mechanism of depressive impairment – all five must be assessed for an accurate clinical picture.
Mood & Affect
The core emotional presentation – persistent low mood, tearfulness, emotional blunting, irritability, or an absence of feeling where feeling should be.
- Persistent sadness or emptiness
- Unexplained tearfulness
- Emotional numbness or flatness
- Irritability (especially in youth)
- Hopelessness or helplessness
Anhedonia
Loss of pleasure, interest, and reward-seeking in activities the person previously enjoyed. Considered the most diagnostically specific feature of depression.
- Uncontrollable worry about the fLoss of interest in hobbies
- Food no longer pleasurable
- Social withdrawal and isolation
- No anticipation of enjoyment
- Emotional detachment from others
Cognitive
Impaired concentration, slowed information processing, working memory deficits, and decisional difficulty – the domain most frequently misdiagnosed as ADHD.
- Can’t concentrate or stay on task
- Slowed thinking
- Forgetfulness and memory gaps
- Difficulty making decisions
- Academic or work performance drop
Somatic
Physical symptoms of depression – sleep disruption, fatigue, appetite and weight changes, and psychomotor changes that manifest in the body before mood symptoms appear.
- Persistent fatigue and low energy
- Insomnia or hypersomnia
- Appetite changes / weight shift
- Psychomotor slowing or agitation
- Unexplained physical complaints
Self-Concept
Negative beliefs about the self – worthlessness, excessive guilt, shame, and distorted self-perception. The domain most associated with persistent depressive disorder and suicidal ideation.
- Excessive guilt or self-blame
- Feelings of worthlessness
- Shame and self-loathing
- Thoughts of death or self-harm
- “I am a burden” cognitions
The Cost of Waiting
Depression Screener Report
Depression does not stay static. Left unidentified, it accumulates functional impairment across every life domain – academic, occupational, relational, and physical. The data on untreated duration is unambiguous: every additional year of untreated depression predicts worse treatment outcomes,higher recurrence rates, and greater structural brain change.
Academic trajectory: A meta-analysis of 32 studies found that depression severity predicts a 0.6–0.8 GPA drop per unit increase in PHQ-9 score, independent of socioeconomic status or learning disability status.
Workplace productivity: WHO estimates that depression and anxiety together cost the global economy US$1 trillion per year in lost productivity — with presenteeism (showing up while functionally impaired) accounting for more loss than absenteeism.
Physical health cascade: Untreated depression is an independent risk factor for cardiovascular disease (2–3× risk), diabetes complications, immune dysregulation, and accelerated cellular ageing. It is not purely a “mental” condition.
Recurrence risk: After one depressive episode, the risk of a second is 50%; after two, 80%; after three, 90%. Early identification and treatment significantly reduces recurrence risk.
Domain Impairment Across Untreated Duration
Data indexed from STAR*D 2023 longitudinal follow-up; NIMH-funded functional impairment studies; Bhattacharya et al. cognitive decline meta-analysis 2024. All figures represent progressive impairment without effective intervention.
What Depression Is Mistaken For
Depression’s cognitive and somatic features are routinely misattributed to other conditions – leavingthe underlying depression in place while the wrong treatment is applied. These misattributions are not rare edge cases. They are the statistical norm.
Condition
Shared Surface Signs
The Depression Tell
ADHD
Inattention, distractibility, poor task completion, impulsivity, underperformance at school or work
ADHD inattention is chronic and trait-like; depression inattention has an onset, worsens over time, and is accompanied by anhedonia, fatigue, and mood change. Depression often responds to sleep and mood support; ADHD does not.
Burnout
Exhaustion, disengagement, reduced performance, emotional detachment, cynicism
Burnout resolves substantially with environmental change and rest. Depression persists and deepens regardless of workload. Self-concept distortion – worthlessness, guilt – is a depression feature, not a burnout feature.
Cognitive Decline
Memory problems, slowed processing, word-finding difficulty, reduced executive function, withdrawal
Depression-driven cognitive impairment fluctuates with mood state; neurodegenerative decline does not. “Pseudodementia” – depressive cognitive syndrome — is among the most reversible of all apparent cognitive decline presentations
Anxiety
Avoidance, social withdrawal, concentration difficulty, sleep disruption, irritability, school refusal
Anxiety is characterised by fear-driven hyperactivation; depression by flat disengagement and loss of motivation. 60–70% of people with depression also meet criteria for an anxiety disorder, making co-morbid screening essential.
Chronic Fatigue / CFS
Profound fatigue, post-exertional malaise, cognitive fog, sleep unrestorative, functional impairment
Anhedonia and negative self-concept are not features of CFS; they are core depression features. Both can co-occur. Depression-associated fatigue typically responds to antidepressant treatment; CFS-associated fatigue does not respond to antidepressants alone.
Motivational / Character
Low effort, disengagement, “doesn’t try,” procrastination, social withdrawal, declining grades or output
Motivation is not a character trait — it is a neurobiological output of dopamine and reward circuitry. Depression systematically impairs this circuitry. Framing depression as laziness or attitude delays treatment and causes lasting harm to self-concept.
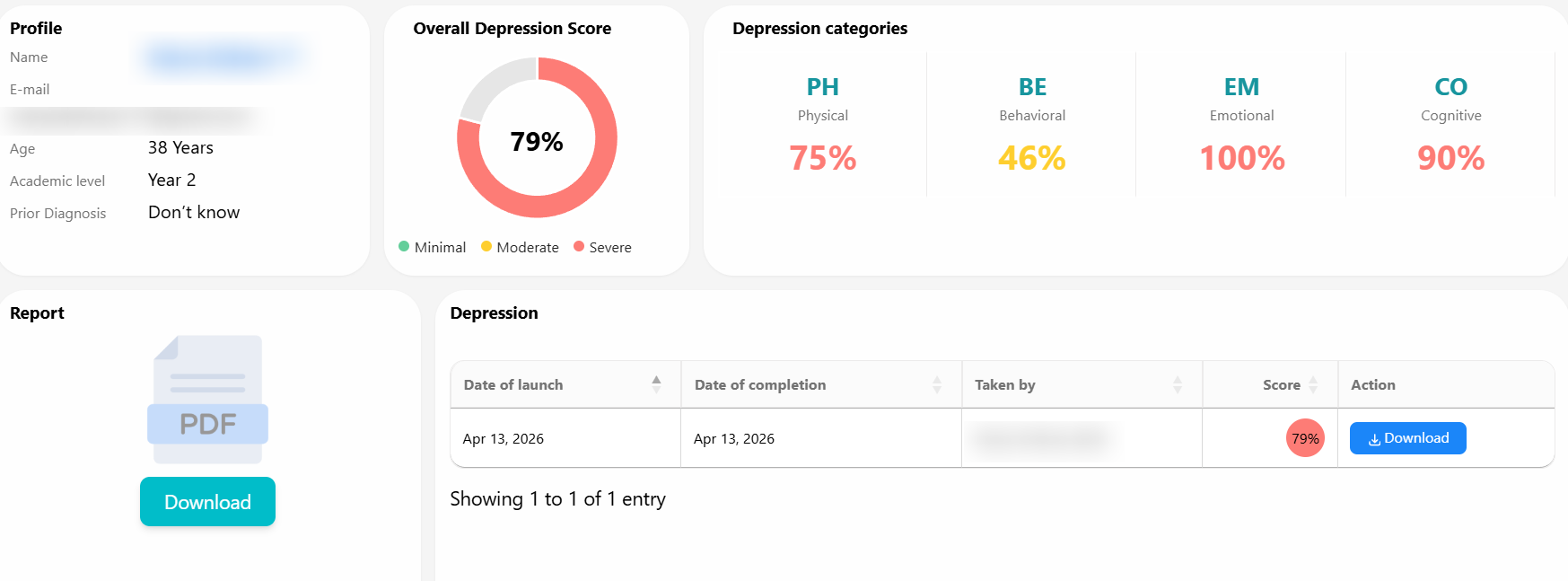
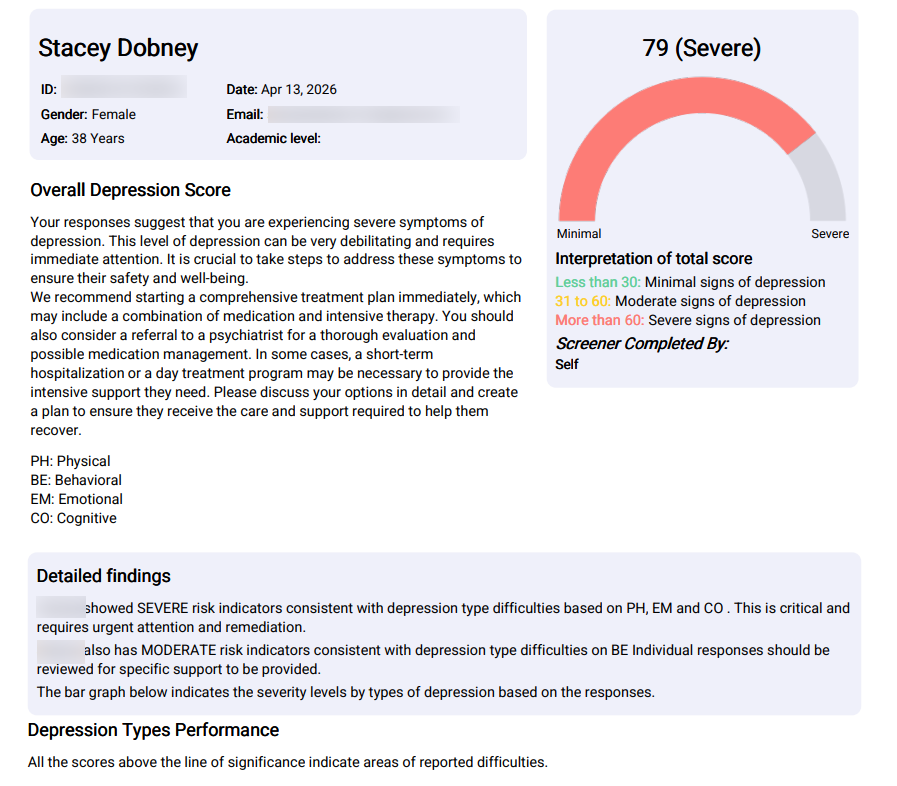
The Depression Screener Report
The MMM Depression Screener produces a structured, multi-domain clinical report. See each section below – this is drawn from an actual sample report (all identifiers redacted).
Sample Report – DEPSCN-DZFQ9MTG
Age: 17 years · Gender: Male · Screener completed by: Self · Date: Dec 11, 2025
The responses suggest severe symptoms of depression across multiple functional domains. This level of depressive impairment is debilitating and requires immediate clinical attention. It is crucial to take steps to address these symptoms to ensure safety and wellbeing.
A comprehensive treatment plan is strongly recommended, including a combination of structured psychotherapy and psychiatric evaluation for medication considerations. A referral to a clinical psychologist or psychiatrist at the earliest opportunity is warranted. The co-occurrence of physical severity and cognitive severity alongside reported self-harm ideation places this presentation in the category requiring urgent professional follow-up – not school-based support alone
Score Interpretation
Domain Interpretation
All scores above the line of significance indicate areas of reported difficulties requiring targeted remediation.
Physical Symptoms (Severe): Significant physical manifestations including persistent sleep disturbances, changes in eating patterns, and severe energy depletion — consistent with neurovegetative features of Major Depressive Disorder.
Cognitive Symptoms (Severe): Marked difficulties in concentration, memory, and decision-making. Consistently reports trouble focusing on tasks, following conversations, and retaining information — significantly impacting academic performance.
Behavioral Symptoms (Moderate): Moderate changes including social withdrawal, decreased participation in activities, and academic avoidance — concerning for both academic and relational outcomes.
Emotional Symptoms (Moderate): Moderate emotional distress characterised by feelings of sadness, worthlessness, and occasional thoughts of self-harm — significant indicators of adolescent depression requiring immediate attention.
Depression Types Performance
All scores above the line of significance indicate areas of reported difficulties requiring targeted remediation.
Targeted Recommendations
Immediate consultation with a mental health professional is strongly recommended, particularly given the presence of thoughts about self-harm and the severe intensity of symptoms.
Establish regular sessions with a school counselor or psychologist to develop coping strategies for managing academic stress and emotional challenges.
Consider a temporary academic accommodation plan to address concentration difficulties and cognitive symptoms while treatment is being initiated.
Implement a structured daily routine that includes regular sleep schedules, balanced meals, and moderate physical activity to help regulate physical symptoms.
Engage in stress-reduction techniques suitable for teenagers, including mindfulness exercises, guided relaxation, and physical activity that can be integrated into the school day.
Family involvement in treatment is crucial – parents should be informed about assessment results and actively involved in creating a supportive home environment.
Monitor for potential co-occurring conditions such as anxiety disorder or attention difficulties, which commonly present alongside depression in adolescents.
Consider joining a teen support group or engaging in group therapy to address social withdrawal and build peer connections in a supported environment.
Clinical Impression & Notes
The responses on the MyMemoryMentor Depression Screener place this individual firmly within the Severe range. This self-reported profile warrants serious clinical attention and should not be minimised or deferred.
Domain-Level Findings: Across the four assessed domains, they present with Severe impairment in both Physical and Cognitive functioning. Physically, they endorsed persistent disruptions to sleep, appetite, energy, and psychomotor activity — a combination strongly associated with neurovegetative features of Major Depressive Disorder. Cognitively, they report consistent difficulties with focus, concentration, memory, and irritability, which are already measurably affecting academic engagement and daily capacity to function.
The Moderate ratings in Behavioral and Emotional domains are equally concerning in clinical context. Of particular clinical urgency are the emotional responses, which include reported thoughts of self-harm and wishes to not be alive. These disclosures must be treated as a priority safeguarding concern requiring immediate professional follow-up.
Recommendations: It is strongly advised that they (with family support) arrange an in-person consultation with a qualified Clinical Psychologist or Psychiatrist at the earliest opportunity. A face-to-face evaluation is essential to conduct a thorough risk assessment, explore the nature and frequency of self-harm ideation, and determine an appropriate level of care which may include structured psychotherapy (CBT or interpersonal therapy for adolescents), psychiatric review for medication considerations, and a coordinated school-based support plan. Family involvement in this process is not optional – it is clinically essential.
The above notes are based solely on screener data and do not constitute a clinical diagnosis. They are intended to support, not replace, a comprehensive in-person psychological evaluation.
Structured Insight Across the Lifespan
The MMM Depression Screener serves parents, educators, clinicians, and individuals – each with a different need, all served by the same structured five – domain report.
Parents & Caregivers
Your teenager has gone quiet. They’ve stopped doing things they used to love. They sleep too much or too little. You’re not sure if this is adolescence or something that needs attention. The screener gives you structured language to bring to a school counsellor or GP.
Early identification and a clear next step
School Counsellors
A student has been referred for falling grades, social withdrawal, or behavioural changes. Before making assumptions about effort or ability, structured screening helps separate academic struggle from depressive impairment – and generates a domain report you can bring to parents and SEN coordinators.
Evidence base for referral and accommodation
GPs & Practitioners
Depression presents in your waiting room as fatigue, sleep complaints, concentration problems, and chronic pain. The MMM screener generates a multi-domain severity profile that can anchor your clinical conversation and inform referral decisions – in under 10 minutes.
Structured severity data before the appointment
Young Adults & Students
University performance is dropping. You’ve stopped going out. You’re exhausted but can’t sleep. You don’t feel sad exactly – you feel nothing. The screener helps you name what you’re experiencing and gives you a structured report you can bring to a campus counsellor or GP.
Language for what you’re going through
Employers & HR Teams
A high-performing employee has disengaged. Output has dropped. They’ve become harder to reach. Depression is the leading cause of workplace absence globally. Structured wellbeing screening gives HR a framework that goes beyond survey scores.
Structured support framework for teams
Older Adults & Families
Depression in older adults is frequently misidentified as dementia, grief, or the natural consequences of ageing. The somatic and cognitive domains of the MMM screener are particularly calibrated to capture late-life depressive presentation, where mood symptoms are often secondary to physical and cognitive complaints.
Differentiation from ageing and cognitive decline
Stop Guessing. Start With Structure.
The average gap between first depressive symptoms and first effective treatment is seven to ten years. A structured screener takes ten minutes and produces a report that can anchor a conversation with a teacher, a doctor, or a family member. Begin here.
Making Depression Visible
Frequently Asked Questions
Important: This screener is not a diagnostic tool and is not a substitute for clinical evaluation. It is designed to assist in identifying possible characteristics of depression in a structured manner. All responses selected as ‘Always’ and ‘Often’ must be paid attention to, as they can help establish the specific protocol for comprehensive assessment and remedial support. If you or someone you know is experiencing a mental health crisis or thoughts of self-harm, please contact a mental health professional or emergency services immediately. In India: iCall 9152987821 · NIMHANS 080-46110007 · Vandrevala Foundation 1860-2662-345 (24/7).