301M
people globally suffer from anxiety -4.05% of the world’s population
WHO; Javaid et al. 2023
28%
U.S. adults reported anxiety symptoms post-pandemic -up from pre-2020 baseline
Forbes Health / CDC, 2024
5.5%
adolescents aged 15–19 globally meet criteria for an anxiety disorder
WHO Adolescent Mental Health, 2024
32.7%
of U.S. women reported anxiety symptoms -vs 24.4% of men
Statista, 2024
Anxiety is the most common mental health
condition on earth – and the most
frequently mistaken for something else.
52%
rise in adolescent anxiety
1990–2021
The Frontiers in Psychiatry 2024 global burden review found a 52% rise in anxiety incidence among 10–24-year-olds, accelerating sharply post-2019. Females show consistently higher prevalence. The 20–24 cohort carries the heaviest disability-adjusted burden.
20–25%
of students with SLDs
meet clinical anxiety criteria
Mumbai SpLD cohort studies and the 2024 Annals of Dyslexia work confirm: anxiety in students with learning disabilities is not a side effect. It is a core part of the picture – and it mediates academic performance independent of the underlying SLD.
~80%
of ADHD cases involve
co-occurring conditions
The most common companion is anxiety. In adults and women, this overlap is the single largest source of diagnostic error. Many adults treated for “ADHD” for years had anxiety masquerading as inattention all along – or both, with one obscuring the other.
What Is Anxiety?
Anxiety is the body’s threat – response system stuck in the “on” position. Where momentary worry helps performance, sustained anxiety hijacks the systems the brain uses for everything else – attention, working memory, decision – making, sleep, and emotional regulation. The same neural circuits that should be learning, working, and connecting are diverted to monitoring danger that is not there.
This is why anxiety is so easily mistaken for something else. Its surface signs – distractibility, restlessness, irritability, forgetfulness, avoidance, withdrawal – overlap with ADHD, SLDs, autism, depression, and even early dementia. Most people experiencing chronic anxiety do not know that what they are experiencing has a name. They believe they are simply scattered, slow, “bad at school,” “bad at work,” or “losing it.”
Anxiety is highly treatable. CBT, structured intervention, and (where appropriate) medication produce significant gains. The barrier is not treatment. The barrier is identification.
“Anxiety disorders rank as the second foremost contributor to disability – adjusted life years globally – second only to depression. Yet anxiety remains under – screened in academic, occupational, and clinical settings, particularly when its symptoms are mistaken for primary attentional, cognitive, or developmental conditions.”
-Xiong et al., Global Burden of Disease 2022
The Threat Loop
The amygdala fires faster, the prefrontal cortex regulates more slowly. The brain commits cognitive resources to threat that is not there – leaving less available for learning, working, and remembering.
Genetic + Environmental
Heritability runs around 30–40%. The rest is environmental – trauma, chronic stress, sleep deprivation, and (increasingly) the cognitive demands of modern adolescence and work.
Across the Lifespan
Anxiety presents differently at 6, 16, 36, and 76. The same underlying mechanism produces school refusal in childhood, panic attacks in young adulthood, burnout at work, and reversible cognitive confusion in older adults.
Highly Treatable
CBT shows large effect sizes in both children and adults. Medication helps where appropriate. Mindfulness, exercise, and sleep hygiene add meaningful gains. The hardest step is the first: knowing that what is happening has a name.
How Anxiety Actually Presents
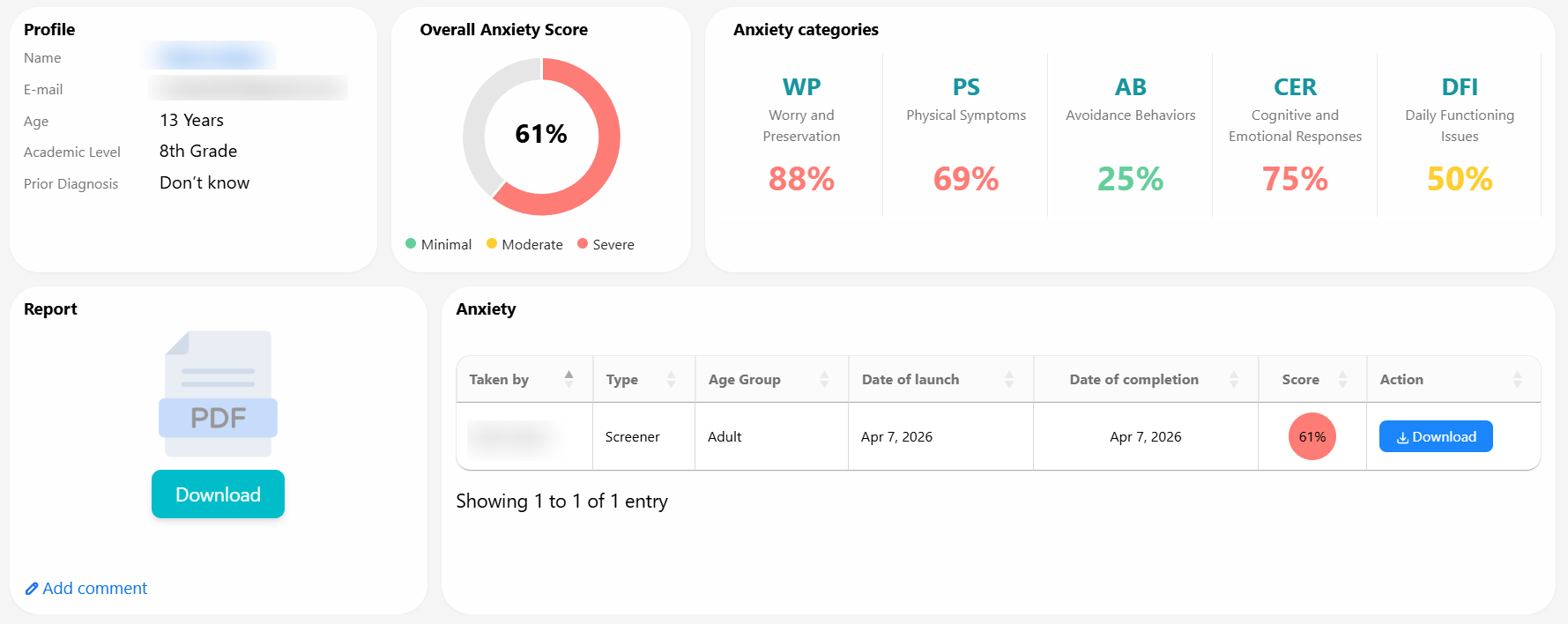
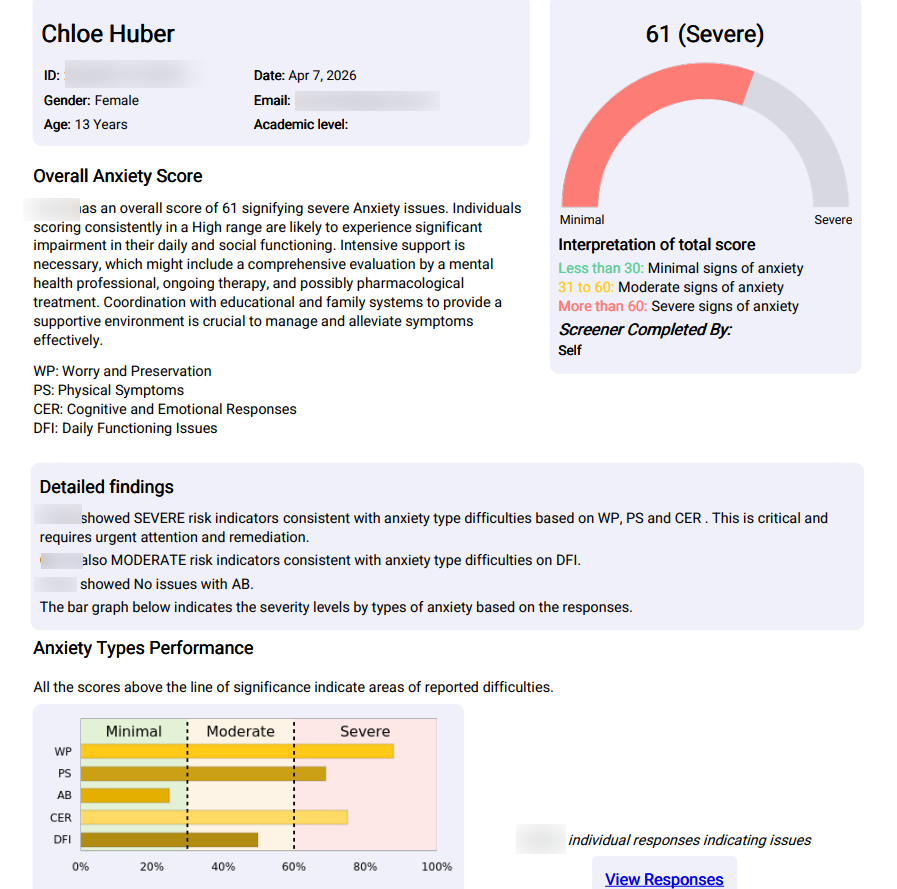
MyMemoryMentor’s anxiety screener does not produce a single score. It produces a five – domain profile – because anxiety is rarely uniform. A learner may be severe in one domain and minimal in another, and the pattern matters more than the total. This is the architecture the screener report uses.
Physical Symptoms
The body’s somatic – autonomic response – heart racing, dizziness, sweating, nausea, breath catching.
- Heart pounding without exertion
- Dizziness or feeling faint
- Tight chest, shallow breathing
- Sweating, hot flushes, nausea
Thought Anxiety
Persistent, intrusive worry – particularly about future events, performance, and worst – case outcomes.
- Uncontrollable worry about the future
- “What if” loops that won’t quiet
- Catastrophic thinking patterns
- Rumination on past mistakes
Social Anxiety
Performance and social situations trigger disproportionate fear – speaking up, group work, presentations.
- Fear of judgement or embarrassment
- Avoidance of group activities
- Severe distress before presentations
- Difficulty making or maintaining friendships
Panic & Fear
Acute episodes of heightened anxiety with both psychological and physical manifestations, often triggered by change.
- Sudden panic attacks
- Fear out of proportion to event
- Distress at unexpected change
- Anticipatory dread before triggers
Behavioral Anxiety
Anxiety expressed through observable behaviour – restlessness, irritability, inability to settle. The domain most often mistaken for ADHD.
- Restlessness, can’t sit still
- Irritability and frustration
- Pacing, fidgeting, leg bouncing
- Difficulty relaxing or winding down
Why Anxiety Gets Misdiagnosed as
Almost Everything Else
Anxiety is the great cognitive imitator. Because chronic worry consumes working memory, hijacks attention, and produces visible restlessness, it looks like ADHD. Because it impairs reading fluency and recall under timed conditions, it looks like an SLD. Because it produces social withdrawal and rigidity, it looks like autism. Because it generates confusion and forgetfulness in older adults, it looks like early dementia. The research on each crossover is settled yet primary screening rarely tests anxiety first.
Condition Anxiety Mimics
Shared Surface Symptoms
What Actually Distinguishes Them
ADHD
Inattention, restlessness, distractibility, irritability, executive function failures, difficulty completing tasks, forgetfulness, fidgeting, “can’t sit still”
ADHD-related inattention is constant and present even during enjoyable activities. Anxiety-driven inattention is situational, triggered by specific worries, and the person is typically aware of their distraction – tense, guilty, hypervigilant.
Specific Learning Disabilities
Slow reading fluency, poor comprehension under time pressure, working memory failures, written expression collapse, mathematical anxiety, test underperformance versus classroom understanding
SLD difficulties are present even in low-stress, untimed conditions. Anxiety-driven academic failure improves dramatically when test conditions change. The 2025 Annals of Dyslexia review confirms test anxiety mediates the relationship between trait anxiety and academic performance independently of any underlying SLD.
Autism Spectrum
Social withdrawal, school refusal, sensory sensitivity, rigidity around routine, meltdowns at change, difficulty with group work, preference for solitude
Autistic social difference is consistent across the lifespan and present from early development. Anxiety-driven social avoidance has a clear onset, fluctuates with stress level, and the person typically wants social connection but cannot access it due to fear, not preference.
Depression
Low energy, poor concentration, sleep disturbance, social withdrawal, irritability, hopelessness, loss of interest in activities, fatigue
Depression centres on sadness, hopelessness, and pervasive low mood. Anxiety centres on fear, dread, and threat. They co-occur frequently – Lancet 2024 places comorbidity around 50% – but the dominant emotional tone differs and matters for treatment selection.
Early Dementia / MCI
Forgetfulness, confusion in new environments, difficulty multitasking, word-finding problems, withdrawal from social activities, slowed processing, “cognitive fog”
Dementia produces progressive, day-to-day cognitive decline that does not fluctuate with mood. Anxiety-driven cognitive confusion fluctuates dramatically with stress level and is reversible. NHATS Round 12 data shows pain, low community cohesion, and depression triggered the anxiety in 51% of older adults flagged with cognitive impairment.
Workplace Burnout
Exhaustion, irritability, cognitive fatigue, depersonalisation, missed deadlines, decision avoidance, late-night ruminating about work, Sunday-evening dread
Burnout is environmentally driven and improves with rest and reduced workload. Anxiety persists even when external demands ease. 61% of workplace caregivers in the 2024 China cohort study reported moderate-to-severe anxiety distinct from their burnout scores.
ADHD
Specific Learning Disabilities
Autism Spectrum
Depression
Early Dementia / MCI
Workplace Burnout
Inattention, restlessness, distractibility, irritability, executive function failures, difficulty completing tasks, forgetfulness, fidgeting, “can’t sit still”
Slow reading fluency, poor comprehension under time pressure, working memory failures, written expression collapse, mathematical anxiety, test underperformance versus classroom understanding
Social withdrawal, school refusal, sensory sensitivity, rigidity around routine, meltdowns at change, difficulty with group work, preference for solitude
Low energy, poor concentration, sleep disturbance, social withdrawal, irritability, hopelessness, loss of interest in activities, fatigue
Early Dementia / Forgetfulness, confusion in new environments, difficulty multitasking, word-finding problems, withdrawal from social activities, slowed processing, “cognitive fog”
Exhaustion, irritability, cognitive fatigue, depersonalisation, missed deadlines, decision avoidance, late-night ruminating about work, Sunday-evening dread
ADHD-related inattention is constant and present even during enjoyable activities. Anxiety-driven inattention is situational, triggered by specific worries, and the person is typically aware of their distraction – tense, guilty, hypervigilant.
SLD difficulties are present even in low-stress, untimed conditions. Anxiety-driven academic failure improves dramatically when test conditions change. The 2025 Annals of Dyslexia review confirms test anxiety mediates the relationship between trait anxiety and academic performance independently of any underlying SLD.
Autistic social difference is consistent across the lifespan and present from early development. Anxiety-driven social avoidance has a clear onset, fluctuates with stress level, and the person typically wants social connection but cannot access it due to fear, not preference.
Depression centres on sadness, hopelessness, and pervasive low mood. Anxiety centres on fear, dread, and threat. They co-occur frequently – Lancet 2024 places comorbidity around 50% – but the dominant emotional tone differs and matters for treatment selection.
Dementia produces progressive, day-to-day cognitive decline that does not fluctuate with mood. Anxiety-driven cognitive confusion fluctuates dramatically with stress level and is reversible. NHATS Round 12 data shows pain, low community cohesion, and depression triggered the anxiety in 51% of older adults flagged with cognitive impairment.
Burnout is environmentally driven and improves with rest and reduced workload. Anxiety persists even when external demands ease. 61% of workplace caregivers in the 2024 China cohort study reported moderate-to-severe anxiety distinct from their burnout scores.
The research is clear and converging. Marsh et al. (Florida State, 2025) demonstrated that domain-general anxiety directly impairs phonological short-term memory in children regardless of whether ADHD is present – cmeaning anxiety produces working memory deficits that look identical to ADHD-driven ones on standardised cognitive testing. Eysenck’s cognitive interference theory, validated in five decades of replication, shows that worry and intrusive thoughts compete for the same working memory resources required for reading, calculation, and learning. The implication is operational: screening for anxiety first, before assuming a primary cognitive or developmental condition, is the single most cost-effective diagnostic step a parent, educator, or clinician can take.
Sources: Marsh et al. 2025 (Frontiers in Psychiatry); Eysenck et al. cognitive interference theory; Annals of Dyslexia 2025; ADHD Evidence Project 2025; Pastor-Cerezuela et al. 2020.
How Common Is Anxiety?
Anxiety is the most common mental health condition globally – and the most rapidly rising in young populations. Yet under 30% of those experiencing it receive anytreatment, and a substantial fraction are misdiagnosed before reaching the right one.
4.4%
global prevalence of anxiety disorders in children aged 10–14
WHO, 2024
5.5%
global prevalence in adolescents aged 15 – 19 – rising sharply post-2019
WHO Adolescent Mental Health 2024
17%
regional prevalence in Australia among adults – among the highest worldwide
AIHW Mental Health
~50%
co-occurrence with depression in adults -the most common comorbid pair
Lancet Commission on Youth Mental Health 2024
How Anxiety Shows Up at Every Age
Anxiety is not a single-stage condition. It changes face across childhood, adolescence, adulthood, and older age – producing the same underlying disruption through entirely different surface symptoms. Identification looks different at each stage. The screening signal does not.
Children – How Anxiety Hides in School
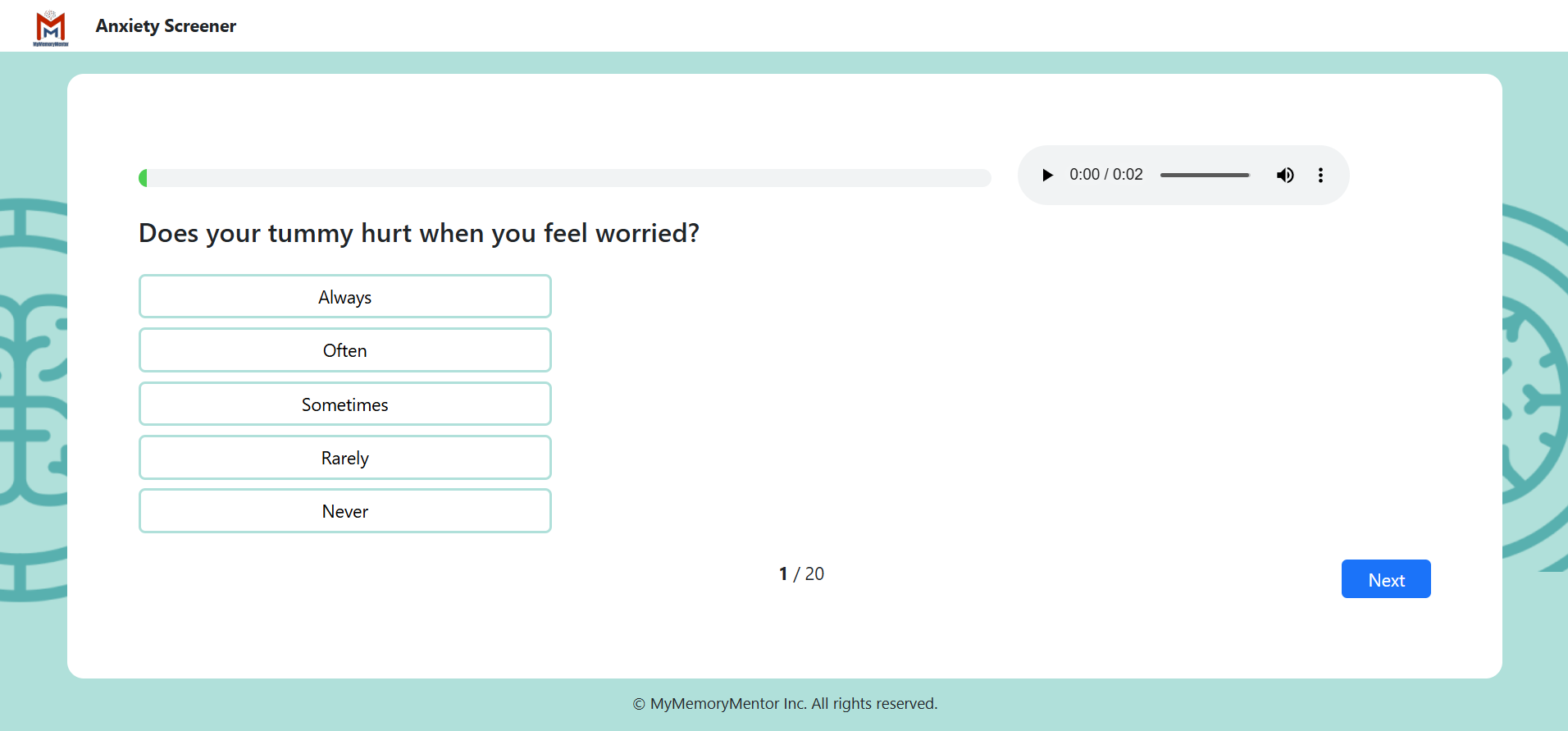
Childhood anxiety rarely arrives saying its own name. It comes as stomach aches on school mornings, tears before homework, refusal to attend birthday parties, separation distress that does not fade with age, and a child who “knows the material but freezes on the test.” Parents and teachers see behaviour. The anxiety underneath stays invisible.
Physical complaints on school mornings — stomach aches, headaches, nausea
Tearfulness or panic before tests, presentations, or new activities
Excessive worry about parents’ safety, separations, sleepovers
Avoidance of activities other children enjoy
“Knows it at home, freezes at school” — performance gap
Sleep difficulties, frequent nightmares, bed-wetting regression
Perfectionism, intolerance of mistakes, eraser-shredded homework
Reported Anxiety Markers in Children
Teens — When School Refusal Begins
Adolescent anxiety is the fastest-growing mental health crisis of the decade. The 2024 Frontiers in Psychiatry global burden review confirmed a 52% rise in incidence from 1990 to 2021, accelerating post-2019. By 15–19, prevalence reaches 5.5% globally – and bullying victimisation has emerged as a major modifiable risk factor.
School refusal – physical inability to enter the building
Persistent rumination, racing thoughts, “what if” loops
Social withdrawal from previously enjoyed friendships
Sudden grade decline without identifiable academic cause
Panic attacks – racing heart, breathing difficulty, dread
Compulsive phone or social media use as escape, not connection
Self-harm or disordered eating as regulation strategies
Adolescent boys may show through anger, withdrawal, substance use
Adolescent Anxiety Self-Reported Impact
Adults — The Cost in the Workplace
Adult anxiety reshapes careers without anyone noticing. It produces Sunday-evening dread, the inability to read long documents, the meeting where everything was understood but nothing could be said, the missed promotion routed around fear of leadership exposure. Adults with anxiety are often labelled cautious, perfectionist, or simply “not management material.” The cost compounds across decades.
Sunday-evening dread, Monday-morning panic
Avoidance of meetings, presentations, public visibility
Procrastination on tasks that produce anxiety, not on all tasks
Email inbox dread – opening messages becomes a daily battle
Career paths unconsciously routed around exposure to fear triggers
Insomnia, particularly mid-night waking with racing thoughts
Decision fatigue and analysis paralysis on routine choices
“High-functioning” anxiety hiding behind perfectionism and over-work
Adult Anxiety Workplace Impact
Older Adults — When Anxiety Looks Like Dementia
Older-adult anxiety is the most misdiagnosed presentation of all. NHATS Round 12 data shows that anxiety in older adults produces forgetfulness, confusion, and cognitive fog that fluctuate with stress level — meaning they reverse with treatment. Dementia does not reverse. Yet many older adults are referred straight to dementia evaluation, when an anxiety screen could have resolved the case.
Cognitive fog that fluctuates with stress, sleep, and medication
Confusion in new environments – supermarkets, social events
Persistent worry about medications, finances, family safety
Withdrawal from social activities once enjoyed
Sleep disturbance with mid-night ruminating
Physical complaints with no medical explanation
Suspected dementia that fluctuates — better days, worse days
Caregiver burnout creating compounding anxiety on top of grief
Older Adult Anxiety Patterns
Why Anxiety Wrecks Cognitive Output
Three converging mechanisms explain how anxiety produces the cognitive signature that gets misdiagnosed as ADHD, SLDs, or early dementia. Each is supported by replicated cognitive neuroscience.
01
Working Memory Hijack
Eysenck’s cognitive interference theory, replicated for five decades, shows that worry and intrusive thoughts compete for the same phonological short-term memory resources required for reading, mental calculation, and learning. Marsh et al. (2025) confirmed this effect operates independently of ADHD – meaning anxiety alone produces working memory deficits that look identical to ADHD on cognitive testing.
The workspace, occupied by worry02
Attentional Bias Toward Threat
The anxious brain preferentially scans for danger. Attention locks onto threat-relevant cues (a teacher’s frown, a vague email, an unexpected phone call) at the expense of task-relevant ones. From outside, this looks like distractibility. From inside, the attention is intensely focused – just on the wrong thing. ADHD’s distraction is content-neutral. Anxiety’s is content-specific.
Focus on the wrong signal03
Autonomic Load on Cognition
Sustained sympathetic nervous system activation – racing heart, shallow breathing, muscle tension – diverts physiological resources to threat preparation. The prefrontal cortex, the region governing complex reasoning and impulse control, receives less. Decisions slow, mistakes rise, and the appearance of cognitive impairment emerges. The cognition was never the problem.
The body, fighting the mindAnxiety Rarely Travels Alone
Anxiety is the most common companion to almost every other mental health and developmental condition. This is not a coincidence. The same neural systems that make a brain vulnerable to ADHD, autism, depression, or learning differences also make it vulnerable to chronic threat response.
The clinical implication is concrete: where anxiety co-occurs with another condition, treating one without the other produces incomplete results. Where anxiety presents alone but is misdiagnosed as another condition, treatment misses the target entirely. Screening for both – and reading the profile carefully – is the only reliable starting point.
~80%
of ADHD cases involve a co-occurring condition -anxiety is the most common
~40%
of autistic children meet criteria for clinically significant anxiety
~50%
of adults with anxiety also experience depression – the most common adult comorbid pair
EMA – Evaluation of Math Ability
A 360° cognitive profile of mathematical learning. For families investigating whether academic struggle is anxiety-driven or rooted in a learning difference, EMA serves a critical diagnostic purpose: it isolates the cognitive systems anxiety hijacks, so the underlying pattern becomes visible.
Why EMA matters in anxiety investigation: Math is the academic subject most reliably disrupted by anxiety. Math anxiety is a documented clinical entity. A child whose number sense and reasoning are intact but whose timed fluency collapses under test conditions is showing the cognitive signature of anxiety – not dyscalculia. EMA’s six-domain profile tells you which.
Number Sense
Foundational understanding of quantities, order, and numerical relationships.
→ Typically intact in anxiety – strong here with timed weakness elsewhere is highly signalling
Math Facts & Fluency
Automatic retrieval of basic operations – the system anxiety hijacks first.
→ Where math anxiety produces its largest measurable effect
Visual Processing & Subitising
Visual-spatial and pattern skills for quantity perception.
→ Generally preserved in anxiety, differentiating it from dyscalculia
Working Memory
Capacity to hold and manipulate numbers during multi – step problems.
→ The exact system Eysenck’s interference theory identifies as anxiety’s primary cognitive cost
Math Reasoning
Application of concepts in untimed word problems and conceptual tasks.
→ Strong reasoning paired with collapsed fluency is the anxiety signature
Rapid Automatised Naming
Speed of visual-verbal association under timed pressure.
→ Anxiety-driven RAN deficits are reversible; SLD-driven deficits are not
The Diagnostic Power of a Cognitive Profile
The anxious brain produces a recognisable pattern on cognitive assessment: strong reasoning under low-pressure conditions, collapse under timed conditions; intact conceptual understanding paired with broken procedural fluency; visual processing intact, working memory consumed by worry. This profile is the inverse of an SLD profile, which shows consistent difficulty across conditions.
EMA captures exactly this distinction across number sense, math facts and fluency, visual processing and subitising, working memory, math reasoning, and rapid automatised naming. When EMA results show high conceptual scores paired with timed-condition collapse and RAN deficits, anxiety becomes the leading hypothesis – and a referred-out clinical confirmation becomes the right next step. The screener flags the signal. EMA confirms the pattern. The right intervention follows.
What Actually Helps
Anxiety is one of the most treatable conditions in mental health. Evidence converges on asmall number of interventions with consistently strong effect sizes – CBT first, with medication,structured environment, and lifestyle scaffolding as essential supporting pieces.
01
Cognitive Behavioural Therapy
The strongest evidence base in mental health. CBT for anxiety produces large effect sizes in both children and adults, with gains maintained at 12 – month follow-up. The first-line intervention for almost every anxiety presentation.
02
Graded Exposure
Avoidance reinforces anxiety; structured, gradual exposure to feared situations rewires the threat response. Particularly effective for social anxiety, specific phobias, and panic disorder.
03
Mindfulness and Body Regulation
Breath work, progressive muscle relaxation, mindful walking, brief meditation. These do not eliminate anxiety – they teach the nervous system to recover faster from spikes, which dramatically reduces functional impact.
04
Medication, When Indicated
SSRIs are first-line for moderate-to-severe presentations. Short-term benzodiazepines have a place in acute crisis but require careful prescribing. Always clinician-led; never replaces psychological intervention.
05
School and Workplace Accommodation
Predictable routines, advance notice of change, alternative presentation formats, quiet regulation spaces, exam accommodations. Recognised under IDEA, the Equality Act 2010, and ADA when functional impairment is documented.
06
Sleep, Exercise, Caffeine, Alcohol
Not cures, but powerful amplifiers. Consistent sleep, daily aerobic movement, reduced caffeine, and managed alcohol use all materially reduce baseline anxiety. Often the first interventions to try, alongside professional support.
Anxiety Screening & Assessment
From a quick free five-domain anxiety profile to EMA, MyMemoryMentor’s comprehensive cognitive assessment that helps disentangle anxiety from learning difference -choose what fits your situation.
Free Anxiety Screener
A validated five-domain anxiety questionnaire that maps to the dimensions clinical assessment investigates: Physical Symptoms, Thought Anxiety, Social Anxiety, Panic & Fear, and Behavioral Anxiety. Produces a structured profile, not a single score.
- Free – no account required to start
- Five-domain breakdown matching clinical practice
- Age-banded versions: child, adolescent, adult, older adult
- Results with plain-language interpretation in under 10 minutes
- Flags differential diagnostic considerations (ADHD, depression, SLD)
- DSM-5 and ICD-11 aligned criteria
MOST COMPREHENSIVE
EMA -Evaluation of Math Ability
MyMemoryMentor’s comprehensive cognitive assessment. Particularly powerful for anxiety investigation when academic struggle needs to be separated from underlying learning difference -surfaces the cognitive fingerprint anxiety leaves on mathematical output.
- Six cognitive domains: number sense, fluency, visual processing, working memory, reasoning, RAN
- Reveals the anxiety signature in academic output
- Distinguishes anxiety-driven from SLD-driven academic failure
- Identifies co-occurring conditions alongside anxiety
- Suitable for IEP, 504, EHCP, and MTSS/RTI submissions
- GDPR and HIPAA-aligned data handling
- Parent- and teacher-friendly report language
Before the next label, the next medication, the next assumption – screen for anxiety first.
A free five-domain anxiety profile takes less than 10 minutes. For families and clinicians investigating academic, workplace, or cognitive struggle, ruling out anxiety is the cheapest, most informative diagnostic step available. EMA adds the cognitive profile that confirms or rules out an underlying SLD.