70%
of children with language processing disorders have concurrent working memory deficits – creating a dual barrier to reading and written expression
Catts et al., 2023; ASHA Language Processing Review
2–3 yrs
average delay before a child with working memory impairment receives any formal cognitive assessment in the US school system
NASP; National Center for Learning Disabilities 2024
67%
of children referred for ADHD evaluation have co-occurring memory or language processing profiles that modify the clinical picture
Willcutt et al., 2022; Barkley ADHD EF meta-analysis
3–4×
greater academic improvement when memory-informed teaching strategies are added alongside standard SpLD intervention
Alloway & Alloway; Gathercole WM Classroom Research, 2023
Memory is not one thing. And when it fails,
children are almost never the ones at fault.
80%
of children with dyslexia have working memory deficits
Working memory and phonological processing share overlapping neural architecture. The Gathercole & Alloway research base (replicated across 20+ longitudinal studies) confirms that working memory is the single strongest predictor of academic achievement in the primary years – stronger than IQ, stronger than attention rating scales.
85%
of children with ADHD show impaired working memory
ADHD is frequently framed as an attention disorder. The emerging consensus from Barkley, Willcutt, and the NIMH is that it is better understood as an executive function and working memory disorder – one where inattention is downstream of the memory failure, not its cause. Treating only attention while ignoring the memory profile produces incomplete outcomes.
1 in 10
children has a working memory impairment significant enough to affect classroom learning
Alloway & Alloway’s population screening data, replicated in UK and US cohorts, shows that approximately 10% of school-age children have working memory capacity below the range needed to keep pace with typical classroom instruction. Most are not identified. Most are described as inattentive, unmotivated, or low-achieving.
What Is Memory Health – in Children and Learning?
Memory health is not about how much a child can memorise. It is the combined efficiency of multiple cognitive systems – working memory (holding and manipulating information in the moment), episodic memory (retaining experiences and events), semantic memory (storing word meanings and concepts), and procedural memory (skills and routines) – working together to support learning, communication, and daily functioning.
In children and adolescents, memory health problems almost never exist in isolation. They are consistently co-occurring with or masquerading as dyslexia, ADHD, developmental language disorder, dyscalculia, dysgraphia, and autism spectrum profiles. The memory difficulties are frequently the underlying mechanism – the reason the SLD manifests as it does — not a separate condition layered on top.
This is why memory health screening belongs at the beginning of any SpLD evaluation pathway, not after months of intervention have failed. A four-domain profile separates which memory systems are affected – and which are intact – producing a clinical picture that is genuinely informative for remediation planning.
“Working memory is one of the most important predictors of a child’s success in school. It underpins the ability to learn to read, to acquire number skills, and to develop the basic building blocks for all academic learning. Children with poor working memory are at high risk of educational failure.”
– Gathercole & Alloway, Working Memory and Learning: A Practical Guide for Teachers (2008) — foundational research replicated through 2024
Working Memory
Holds and manipulates information in real time. The bottleneck for reading comprehension, mental arithmetic, and following multi-step instructions.
Episodic Memory
Stores personal events and temporal sequences. Disruptions here produce forgetfulness about recent events, appointments, and learned material.
Semantic Memory
Stores word meanings, concepts, and world knowledge. Word-finding difficulties and vocabulary gaps often reflect semantic memory access problems.
Prospective Memory
Remembering to do future tasks and intentions. Impairments produce the “forgets to hand in homework” and “loses everything” pattern misread as carelessness.
Four Domains of Memory Health
The MMM Memory Health Screener assesses four evidence-based domains drawn from neuropsychological research on childhood memory and cognitive functioning. Each domain maps to distinct neural systems – enabling a profile that is granular enough to guide targeted support rather than generic intervention.
Memory & Recall
The core encoding and retrieval system – whether information is stored and whether it can be reliably accessed on demand. The most diagnostically significant domain for learning difficulties.
- Forgets recent events (lunch, conversations)
- Loses belongings repeatedly
- Cannot recall significant past events
- Forgets names of familiar people
- Cannot remember multi-step instructions
- Inconsistent performance (knows it, then doesn’t)
Orientation & Spatial Awareness
Temporal orientation (time, dates, sequences), spatial navigation, and environmental awareness. Intact OSA rules out global disorientation; impairment signals deeper neurological concern.
- Gets lost in familiar places
- Loses track of time and date
- Confuses sequence of events
- Difficulty with maps, directions
- Disoriented in new environments
- Cannot retrace steps or routes
Language & Communication
Word retrieval, verbal fluency, naming, and language processing – the interface between memory and expression. Co-elevation with MAR is the most clinically significant pattern for SpLD identification.
- “Tip of the tongue” word failures
- Difficulty naming common objects
- Grammatical errors in writing
- Repeats questions or stories shortly after
- Substitutes vague words (“thing,” “that”)
- Difficulty following complex verbal directions
Executive Function & Judgment
Planning, decision-making, inhibition, and safety awareness – the metacognitive layer that governs how memory systems are deployed. EFJ impairment without MAR severity often points to ADHD-inattentive or frontal lobe processing profiles.
- Forgets to turn off appliances / lock doors
- Difficulty making simple daily decisions
- Poor planning and task sequencing
- Impulsive choices with poor judgment
- Cannot manage multi-step tasks
- Reduced safety awareness and risk assessment
Memory Health & the SpLD Landscape
Memory difficulties rarely exist in isolation. They are structurally embedded in the neurodevelopmentalprofiles associated with specific learning differences. Understanding which memory domains are impaired – and which are intact – is what converts a vague “memory problem” into an actionable clinical picture that informs SpLD identification, school accommodation, and remediation planning.
Condition
Memory Mechanism Implicated
What the MMM Profile Reveals
Dyslexia
Phonological working memory impairment and verbal short-term memory weakness – specifically, the phonological loop component of Baddeley’s working memory model. Children cannot hold sound sequences long enough to decode unfamiliar words.
Elevated MAR + LAC with intact OSA. The MAR-LAC co-elevation distinguishes dyslexia-associated memory from global memory disorder. Targeted phonological working memory training has the strongest evidence base for reading improvement in this profile.
ADHD
Central executive working memory impairment – difficulty inhibiting irrelevant information and updating working memory contents in real time. Barkley’s extended phenotype model positions ADHD as fundamentally a failure of working memory for the future (prospective memory).
Elevated EFJ ± MAR with intact or borderline LAC and OSA. The EFJ-dominant profile distinguishes ADHD-type memory failure from language processing disorder. Critically, medication normalises arousal but often leaves working memory capacity partially unaddressed – requiring explicit strategy training.
Developmental Language Disorder
Verbal working memory and phonological processing deficits that impair the storage and manipulation of language-based information. Sentence recall and verbal fluency tasks are particularly sensitive to DLD-associated memory dysfunction.
Elevated LAC, often with concurrent MAR elevation. Intact OSA and EFJ helps distinguish DLD from broader neurodevelopmental profiles. Speech-language therapy targeting verbal working memory strategies (rehearsal, chunking, imagery) produces the largest gains in this domain pattern.
Dyscalculia
Visuospatial working memory impairment – difficulty holding and manipulating numerical and spatial information in working memory simultaneously. Place value, multi-digit operations, and geometry all rely heavily on this component.
Elevated OSA (spatial component) ± MAR. The OSA domain of the MMM screener captures the spatial orientation aspect of this profile. Children with dyscalculia-type memory rarely have language or episodic memory elevation – this specificity guides the remediation toward spatial-numerical strategies rather than language-based approaches.
Autism Spectrum
Atypical memory profiles – strong rote/procedural memory with selective episodic memory difficulties; relative weakness in social memory (names, faces, conversations) despite strong semantic memory for specialist domains. Executive memory (prospective, contextual) is frequently impaired.
Mixed profiles – elevated EFJ with variable MAR, typically intact or above-average OSA. The profile asymmetry (strong in some domains, weak in others) helps distinguish autism-related memory from global impairment. Strategies that leverage preserved semantic and procedural memory are significantly more effective than general memory training.
Dysgraphia
Procedural memory and motor-orthographic mapping – difficulty automatising the motor sequences for letter formation, which occupies working memory capacity that should be available for composition. The cognitive load of physically writing leaves no working memory available for generating content.
MAR elevation (retrieval) combined with EFJ (task management) in the context of written expression difficulties. OSA and LAC typically intact or near-intact. Accommodations that offload motor demands (typing, voice-to-text, scribe) directly free working memory capacity – not an accommodation around the difficulty but a treatment of its underlying mechanism.
Dyslexia
ADHD
Developmental Language Disorder
Dyscalculia
Autism Spectrum
Dysgraphia
Phonological working memory impairment and verbal short-term memory weakness – specifically, the phonological loop component of Baddeley’s working memory model. Children cannot hold sound sequences long enough to decode unfamiliar words.
Central executive working memory impairment – difficulty inhibiting irrelevant information and updating working memory contents in real time. Barkley’s extended phenotype model positions ADHD as fundamentally a failure of working memory for the future (prospective memory).
Verbal working memory and phonological processing deficits that impair the storage and manipulation of language-based information. Sentence recall and verbal fluency tasks are particularly sensitive to DLD-associated memory dysfunction.
Visuospatial working memory impairment – difficulty holding and manipulating numerical and spatial information in working memory simultaneously. Place value, multi-digit operations, and geometry all rely heavily on this component.
Atypical memory profiles – strong rote/procedural memory with selective episodic memory difficulties; relative weakness in social memory (names, faces, conversations) despite strong semantic memory for specialist domains. Executive memory (prospective, contextual) is frequently impaired.
Procedural memory and motor-orthographic mapping – difficulty automatising the motor sequences for letter formation, which occupies working memory capacity that should be available for composition. The cognitive load of physically writing leaves no working memory available for generating content.
Elevated MAR + LAC with intact OSA. The MAR-LAC co-elevation distinguishes dyslexia-associated memory from global memory disorder. Targeted phonological working memory training has the strongest evidence base for reading improvement in this profile.
Elevated EFJ ± MAR with intact or borderline LAC and OSA. The EFJ-dominant profile distinguishes ADHD-type memory failure from language processing disorder. Critically, medication normalises arousal but often leaves working memory capacity partially unaddressed – requiring explicit strategy training.
Elevated LAC, often with concurrent MAR elevation. Intact OSA and EFJ helps distinguish DLD from broader neurodevelopmental profiles. Speech-language therapy targeting verbal working memory strategies (rehearsal, chunking, imagery) produces the largest gains in this domain pattern.
Elevated OSA (spatial component) ± MAR. The OSA domain of the MMM screener captures the spatial orientation aspect of this profile. Children with dyscalculia-type memory rarely have language or episodic memory elevation – this specificity guides the remediation toward spatial-numerical strategies rather than language-based approaches.
Mixed profiles – elevated EFJ with variable MAR, typically intact or above-average OSA. The profile asymmetry (strong in some domains, weak in others) helps distinguish autism-related memory from global impairment. Strategies that leverage preserved semantic and procedural memory are significantly more effective than general memory training.
MAR elevation (retrieval) combined with EFJ (task management) in the context of written expression difficulties. OSA and LAC typically intact or near-intact. Accommodations that offload motor demands (typing, voice-to-text, scribe) directly free working memory capacity – not an accommodation around the difficulty but a treatment of its underlying mechanism.
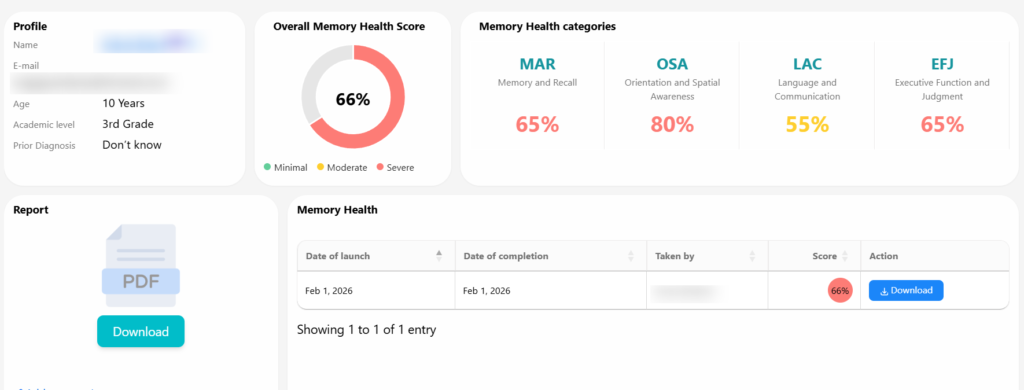
The Memory Health Screener Report
The MMM Memory Health Screener produces a structured four-domain clinical report with domain severity scores, individual response flags, targeted recommendations, and a practitioner-facing clinical note. This is drawn from a real sample report (all identifiers redacted).
Sample Report – Memory Health Screener
Age: 12 years · Gender: Female · Screener completed by: Parent · Date: Feb 2, 2026
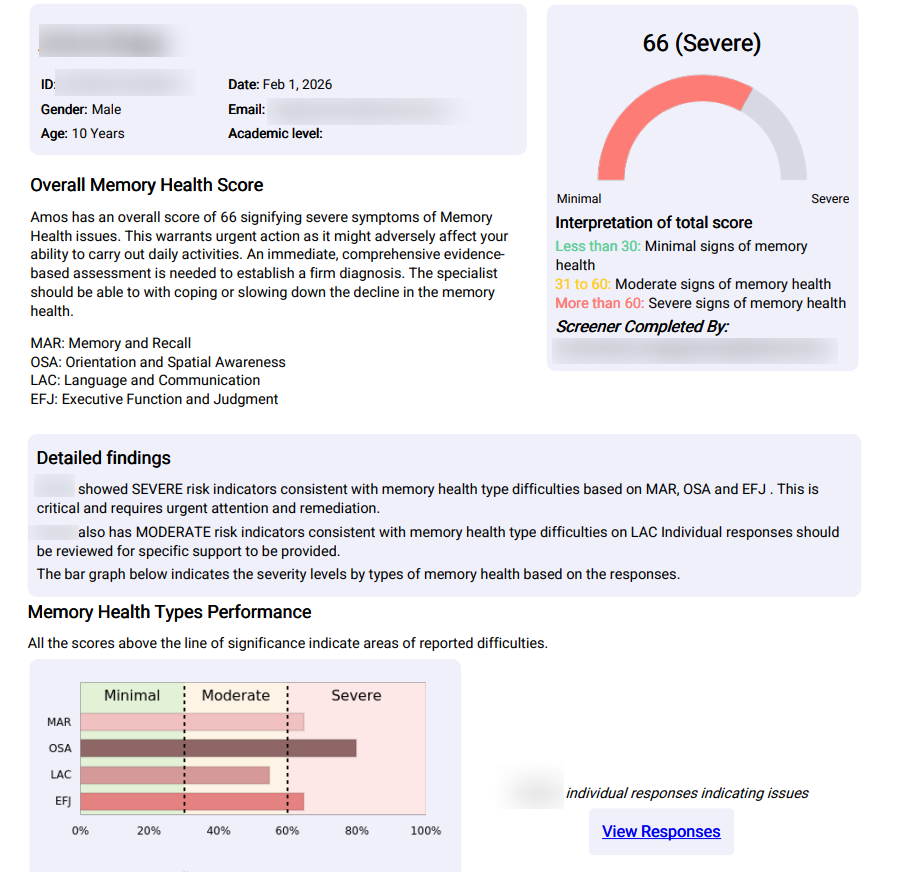
An overall score of 41 signifies moderate symptoms of Memory Health difficulties. This warrants closer observation, additional assessment, and reaching out to a specialist to understand the causes and remediation of the specific memory challenges. A moderate score should not be minimised – moderate memory health impairment at age 12 carries significant academic and functional implications if left unaddressed.
Severe risk indicators are present in the Memory and Recall (MAR) domain, which is critical and requires urgent attention. Moderate risk indicators are present in Language and Communication (LAC) and Executive Function and Judgment (EFJ). Orientation and Spatial Awareness (OSA) shows no significant issues — a clinically reassuring finding that rules out global disorientation or acute neurological concern.
Score Interpretation
Domain Interpretation
Memory and Recall (Severe): Significant challenges remembering recent events, frequently misplacing objects, difficulty recalling significant past events, and sometimes forgetting familiar names. At age 12, these challenges may indicate developing difficulties with working memory and episodic memory formation impacting academic learning and daily functioning.
Language and Communication (Moderate): Often struggles to find the right words when speaking, difficulty naming common objects, makes grammatical errors in writing, and repeats questions within short periods. These language processing challenges affect verbal expression and word retrieval — important for classroom participation and written assignments.
Executive Function and Judgment (Moderate): Concerning patterns in judgment and safety awareness, forgetting important tasks. Difficulty making simple daily decisions. Planning and problem-solving appear more intact, suggesting executive functioning challenges rather than broad cognitive impairment.
Orientation and Spatial Awareness (No Issues): Intact OSA is clinically reassuring — rules out the kind of global disorientation that would signal acute neurological concern. This selective profile is more consistent with a learning or language processing profile than a neurodegenerative process.
Memory Health Types Performance
All scores above the line of significance indicate areas of reported difficulties requiring targeted remediation.
Targeted Recommendations
Consult with a pediatric neuropsychologist or developmental pediatrician for comprehensive evaluation — these memory and cognitive concerns are atypical for a 12-year-old and require professional assessment to determine underlying causes.
Implement memory support strategies including visual schedules, reminder systems, and structured routines to help with daily tasks and academic responsibilities while formal assessment is pending.
Work with school personnel to develop accommodations: extended time for assignments, written instructions rather than verbal-only directions, and memory aids for classroom activities.
Consider speech-language therapy evaluation to address word-finding difficulties and support language processing skills impacting communication and academic performance.
At school: provide written instructions alongside verbal delivery, allow processing time before expecting responses, and use recognition-based assessments to distinguish what is known from what can be retrieved.
Pursue comprehensive neuropsychological evaluation prioritising working memory, phonological processing, and attention — screen for ADHD-Inattentive type and language processing disorder.
Monitor for potential co-occurring conditions including attention disorders, learning disabilities, or medical conditions that may be contributing to these cognitive challenges.
Clinical Notes – Practitioner Overview
This profile presents a pattern that warrants both clinical attention and interpretive caution. Memory and Recall (MAR) registers Severe; Language and Communication (LAC) and Executive Function and Judgment (EFJ) are Moderate; Orientation and Spatial Awareness (OSA) shows no issues. The intact OSA is clinically reassuring as it rules out the kind of global disorientation that would signal acute neurological concern.
The MAR-LAC co-elevation is the clinically meaningful finding. Word retrieval difficulty alongside memory recall weakness in a 12-year-old frequently points to underlying working memory or language processing deficits rather than a primary memory disorder. This profile is more consistent with a learning disability or attentional difficulty than with a neurodegenerative process. The Severe MAR rating should be interpreted as a directional signal, not definitive severity.
What should happen before formal diagnostic assessment: At home, implement structured routines with visual supports – consistent homework sequences, designated belongings stations, verbal rehearsal strategies (saying instructions aloud before executing). At school, provide written instructions alongside verbal delivery, allow processing time, and use recognition-based assessments alongside recall-based ones.
Pursue comprehensive neuropsychological evaluation prioritising working memory, phonological processing, and attention. Screen for ADHD-Inattentive type and language processing disorder. The memory signal is real. The underlying mechanism needs identification.
Notes are based solely on screener data and do not constitute a clinical diagnosis. They are intended to support, not replace, a comprehensive in-person neuropsychological evaluation.
Structured Insight for Every Pathway
The MMM Memory Health Screener serves parents, educators, clinicians, and individuals – each with a different starting point, all arriving at the same structured four-domain report.
Parents & Caregivers
Your child forgets homework, loses everything, can’t find words mid-sentence, and struggles with instructions that other children seem to handle easily. You’ve been told it’s attention. You’re not sure. The screener produces structured language you can bring to a pediatrician, psychologist, or school team.
Evidence to advocate for assessment
Teachers & School Counsellors
A student is not retaining classroom instruction, has word-finding gaps that affect participation, and produces written work far below their apparent verbal ability. Structured memory screening before referring to the SEN team helps distinguish memory-specific profiles from attentional or motivational ones.
Structured referral data for SEN pathways
Clinicians & Neuropsychologists
Pre-assessment screening that identifies which memory domains to prioritise in formal evaluation. The MAR-LAC co-elevation pattern and OSA baseline guide test battery selection and differential diagnostic priorities before the appointment begins.
Domain triage before formal assessment
Adolescents & Young Adults
You’ve always struggled to retain information despite trying hard, or you lose track of what people are saying mid-conversation, or you can understand content but can’t write it down. You may be heading into higher education with an unidentified working memory profile. The screener gives you a structured starting point.
Self-understanding and accommodation pathway
Speech-Language Pathologists
Language and communication domain data that quantifies the memory contribution to word retrieval and verbal processing difficulties – supporting therapy planning and progress documentation with structured baseline data.
Baseline for therapy target-setting
Special Education Coordinators
IEP and 504 plan development benefits significantly from domain-level memory profiling. Knowing that a student has MAR-LAC co-elevation changes the accommodation set: written instructions, recognition-based testing, processing time, and verbal rehearsal supports – all justified by the domain data.
IEP and 504 plan evidence base
Age-Related Memory & Clinical
Cognitive Assessment – Coming to MyMemoryMentor
The Memory Health Screener currently focuses on learning-related memory in children, adolescents,
and young adults. We are building the next generation of assessment tools for age-related memory
change and clinical cognitive conditions – app-based, evidence-validated, and designed for
self-assessment and clinic use alike.
Age-Related Memory Change
Structured self-assessment for adults 50+ noticing changes in name recall, word finding, multitasking, and everyday memory – distinguishing normal ageing from clinical concern.
Dementia & MCI Screening
App-based and clinic-deployable cognitive assessment for Mild Cognitive Impairment and early-stage dementia – structured domain profiling across memory, orientation, language, and executive function.
Alzheimer’s Assessment Support
Longitudinal cognitive tracking tools for individuals and families navigating an Alzheimer’s diagnosis – structured progress monitoring and caregiver-facing domain reports for care planning.
Traumatic Brain Injury (TBI)
Post-injury cognitive profiling for individuals recovering from mild, moderate, or severe TBI – baseline and longitudinal memory assessment to guide rehabilitation planning and return-to-activity decisions.
Parkinson’s Cognitive Profile
Cognitive assessment tools calibrated to the Parkinson’s disease neuropsychological phenotype – visuospatial memory, processing speed, executive function, and attention profiling for both self-assessment and clinical use.
Be the first to know when clinical cognitive assessments launch on the MyMemoryMentor platform.
Current tools focus on learning-related memory and neurodevelopmental profiles below
Stop Calling It Carelessness. Start With Structure.
Most children with working memory profiles wait two to three years from first teacher concern to first formal assessment. A structured screener takes ten minutes and produces a domain report that changes what happens in the next conversation with a teacher, doctor, or IEP team.
Making Memory Health Visible
Frequently Asked Questions
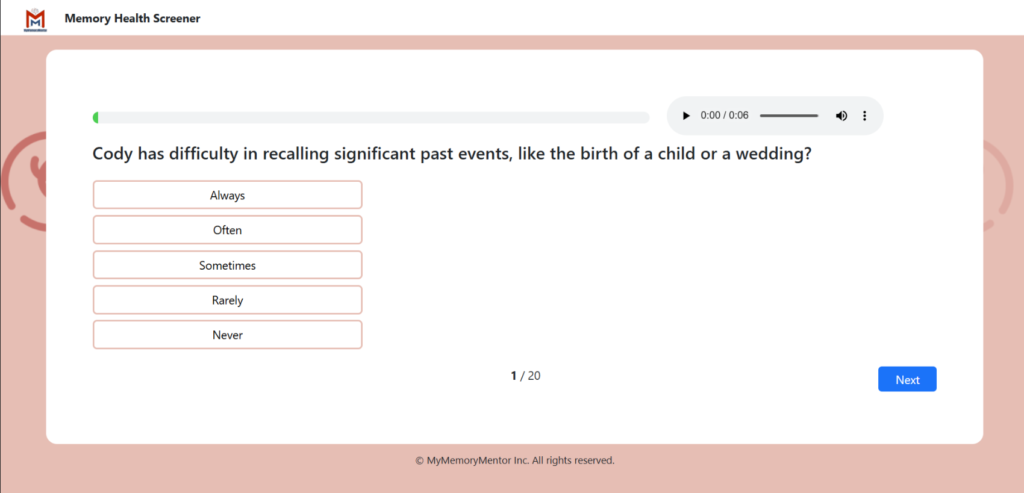
Important: This screener is not a diagnostic tool and is not a substitute for neuropsychological evaluation. It is designed to assist in identifying possible characteristics of memory health difficulties in a structured manner. All responses selected as ‘Always’ and ‘Often’ must be paid attention to, as they can help establish the specific protocol for comprehensive assessment and remedial support. If you have concerns about a child’s memory, please consult a qualified psychologist, neuropsychologist, or developmental pediatrician. US Resources: CHADD (ADHD/memory) 1-800-233-4050 · National Alliance on Mental Illness (NAMI) 1-800-950-6264 · Child Mind Institute childmind.org · Understood.org for learning and memory differences.